Live Now
Cato at Liberty
Cato at Liberty
Cato at Liberty
Cato at Liberty
Topics
Health Care
June 28, 2011 11:41AM
Republicans Getting Rich off ObamaCare
Here we have the spectacle of a former Republican Health and Human Services secretary getting rich by helping states implement ObamaCare. Leavitt Partners (among other consultants) is helping states create the law’s health insurance “Exchanges.” Or the non-ObamaCare-compliant health insurance Exchanges that will by law become ObamaCare-compliant Exchanges. Via Politico:
More than $300 million in exchange grants has already flowed into the states since the Affordable Care Act passed. That number will grow exponentially in the coming months, as states move from the initial steps of passing exchange legislation to the more lucrative task of setting them up.
For health consultants and information technology vendors, it’s already shaping up to be a gold mine…
The opportunity is, seemingly, everywhere. Even in states that have used executive orders and heated rhetoric to push back against implementation of the reform law, vendors still see possible contracts.
“There is a group that feels as though they don’t want to be associated with the Affordable Care Act,” said Leavitt Partners CEO Michael Leavitt, who was Health and Human Services secretary under President George W. Bush. “Privately, though, it’s clear that several of those are planning behind the scenes, because they don’t want to have a federal exchange.”
These Exchanges—there is no such thing as a state-run Exchange—are the government bureaucracies that will make health insurance more expensive, induce employers to drop coverage, entrench ObamaCare, and dole out hundreds billions of debt-financed government subsidies to insurance companies.
Related Tags
June 28, 2011 10:29AM
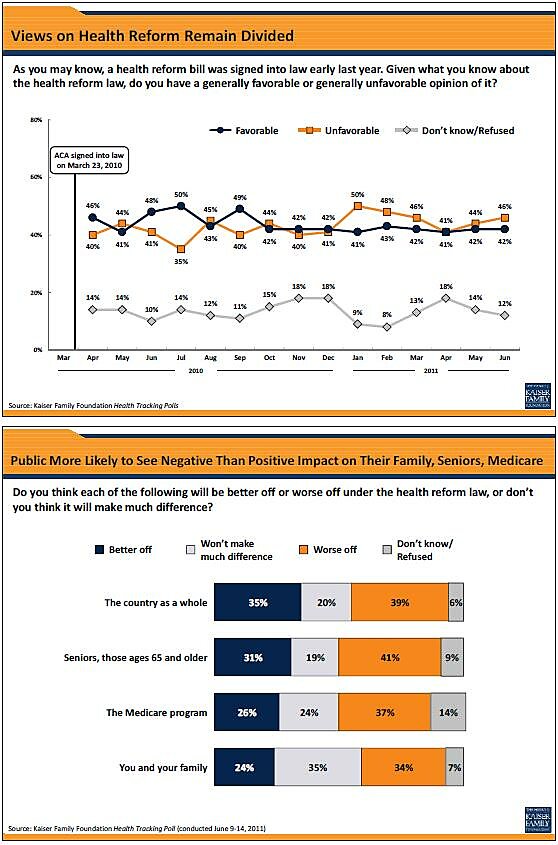
For ObamaCare, June Has Been a Very Cold Month
That’s the subject of my latest Kaiser Health News column:
Obamacare passes two milestones this month. It has been exactly two years since the first version of the legislation appeared in Congress. And it has now enjoyed exactly two years of solid public opposition. Yet this month has been harsher than most.
It is almost enough to make you feel sorry for ObamaCare. Almost.
Related Tags
June 27, 2011 10:55AM
Block-Granting Medicaid Is a Long-Overdue Way of Restoring Federalism and Promoting Good Fiscal Policy
This new video, based in large part on the good work of Michael Cannon, explains why Medicaid should be shifted to the states. As I note in the title of this post, it’s good federalism policy and good fiscal policy. But the video also explains that Medicaid reform is good health policy since it creates an opportunity to deal with the third-party payer problem.
One of the key observations of the video is that Medicaid block grants would replicate the success of welfare reform. Getting rid of the federal welfare entitlement in the 1990s and shifting the program to the states was a very successful policy, saving billions of dollars for taxpayers and significantly reducing poverty. There is every reason to think ending the Medicaid entitlement will have similar positive results.
Medicaid block grants were included in Congressman Ryan’s budget, so this reform is definitely part of the current fiscal debate. Unfortunately, the Senate apparently is not going to produce any budget, and the White House also has expressed opposition. On the left, reducing dependency is sometimes seen as a bad thing, even though poor people are the biggest victims of big government.
It’s wroth noting that Medicaid reform and Medicare reform often are lumped together, but they are separate policies. Instead of block grants, Medicare reform is based on something akin to vouchers, sort of like the health system available for Members of Congress. This video from last month explains the details.
In closing, I suppose it would be worth mentioning that there are two alternatives to Medicaid and Medicare reform. The first alternative is to do nothing and allow America to become another Greece. The second alternative is to impose bureaucratic restrictions on access to health care—what is colloquially known as the death panel approach. Neither option seems terribly attractive compared to the pro-market reforms discussed above.
Related Tags
June 27, 2011 9:01AM
Court Extends Commercial Speech Protections
In an important but little-noted First Amendment case decided Thursday, Sorrell v. IMS Health Inc., the Supreme Court correctly invalidated a particular regulation of commercial speech but unfortunately left intact the general doctrine that distinguishes and privileges noncommercial speech. Justice Kennedy authored the 6–3 decision (joined not just by the “conservatives” but also Justice Sotomayor) that struck down a Vermont law prohibiting the sale of information about doctors’ prescription histories as making viewpoint-based speech restrictions in violation of the First Amendment.
In so ruling, the Court effectively affirmed a Second Circuit decision (involving a similar Connecticut law) I discussed previously. Cato filed amicus briefs in both the Second Circuit and Supreme Court.
The Supreme Court first found that Vermont’s law is subject to heightened scrutiny—not simply the “intermediate” scrutiny typically applied to restrictions on commercial speech—because, on its face, it enacts content- and speaker-based burdens on protected expression. It then rejected the two justifications for the statute the state had asserted: (1) that it is necessary to protect medical privacy, including physician confidentiality, avoidance of harassment, and the integrity of the doctor-patient relationship; and (2) that it is integral to the achievement of policy objectives—namely, improved public health and reduced healthcare costs.
That’s fine as far as it goes, but it leaves open the possibility for broader restrictions on speech, such as if a state wanted to prohibit all prescription-related speech, not just that by data-mining companies to pharmaceutical companies who would use it to tailor their marketing efforts. Our Supreme Court brief, in contrast, argued that the Court should abandon the unworkable distinction between commercial and noncommercial speech established in the 1980 case of Central Hudson Gas & Electric v. Public Service Commission.
The Central Hudson rule should be abandoned in favor of strict scrutiny of all speech restrictions because innovative and valuable commercial expression deserves full First Amendment protection. For more on our preferred approach, see this blogpost.
Still, even as Sorrell v. IMS Health doesn’t entirely eliminate the commercial speech doctrine, the Court does make clear that information—even commercial information sold for commercial purposes—is more than a mere commodity (Vemont had likened it to beef jerky). Commercial speech provides valuable information to the marketplace; by definition, the more such information consumers receive, the better-informed decisions they can make.
I could end my analysis there, but one amusing postscript is that the dissent, written by Justice Breyer and joined by Justices Ginsburg and Kagan, resorts to argument ad Lochneram. That is, just as one should discount any political argument invoking Hitler and Nazis, a legal argument invoking the alleged horrors of the Lochner era (striking down regulations on economic liberty grounds) is inherently suspect. Indeed, Justice Kennedy dismisses Breyer’s concern by noting that while the enactment of “Mr. Herbert Spencer’s Social Statics” is not at issue—alluding to Oliver Wendell Holmes’s Lochner dissent—the duly binding First Amendment is.
In any event, the battle line between the majority and dissent is clear—and it is telling that Justices Sotomayor and Kagan are on opposite sides. (Recall that the scope of First Amendment protection was an issue in Justice Kagan’s confirmation hearings.) If indeed Justice Breyer’s prediction that this decision “opens a Pandora’s Box of First Amendment challenges to many ordinary regulatory practices that may only incidentally affect a commercial message,” this case may have revealed not the views of Justice Kennedy—who is strongly libertarian on speech issues—but the true First Amendment colors of President Obama’s two appointees.
Thanks to Cato legal associate Caitlyn Walsh McCarthy for her help with our briefing and this blogpost.
June 24, 2011 8:37AM
Sorrell vs. IMS Health: Not a Privacy Case
The Supreme Court’s decision in Sorrell vs. IMS Health is being touted in many quarters as a privacy case, and a concerning one at that. Example: Senator Patrick Leahy (D‑VT) released a statement saying “the Supreme Court has overturned a sensible Vermont law that sought to protect the privacy of the doctor-patient relationship.” That’s a stretch.
The Vermont law at issue restricted the sale, disclosure, and use of pharmacy records that revealed the prescribing practices of doctors if that information was to be used in marketing by pharmaceutical manufacturers. Under the law, prescription drug salespeople—“detailers” in industry parlance—could not access information about doctors’ prescribing to use in focusing their efforts. As the Court noted, the statute barred few other uses of this information.
It is a stretch to suggest that this is a privacy law, given the sharply limited scope of its “protections.” Rather, the law was intended to advance the state’s preferences in the area of drug prescribing, which skew toward generic drugs rather than name brands. The Court quoted the Vermont legislature itself, finding that the purpose of the law was to thwart “detailers, in particular those who promote brand-name drugs, convey[ing] messages that ‘are often in conflict with the goals of the state.’ ” Accordingly, the Court addressed the law as a content- and viewpoint-oriented regulation of speech which could not survive First Amendment scrutiny (something Cato and the Pacific Legal Foundation argued for in their joint brief.)
What about patients’ sensitive records? Again, the case was about data reflecting doctors’ prescribing practices, which could include as little as how many times per year they prescribe given drugs. (They probably include more detail than that.) The risk to patients is based on the idea that patients’ prescriptions might be gleaned through sufficient data-mining of doctors prescribing records (no doubt with other records appended). That’s a genuine problem, if largely theoretical given the availability and use of data today. Vermont is certainly free to address that problem head on in a law meant to actually protect patients’ privacy—against the state itself, for example. Better still, Vermonters and people across the country could rely on the better sources of rules in this new and challenging area: market pressure (to the extent possible in the health care area) and the (non-prescriptive, more adaptive) common law.
Whatever the way forward, Sorrell vs. IMS Health is not the privacy case some are making it out to be, it’s not the outrage some are making it out to be, and it’s not the last word on data use in our society.
June 22, 2011 9:20PM
Vouchers in Education and Health Care Reform
E.D. Kain has a post up here (and here) comparing and contrasting vouchers in education and health care. It’s an interesting post that manages both insight and remarkable oversights in a very short space.
And the insight and oversights are bound up with each other:
I think it’s a consistent position to support both single-payer health care – something many progressives advocate – and single-payer education – something many libertarians advocate…
[Medicare] is a lot like what many school choice advocates want. They want government to foot the bill, but they don’t want them to provide the service, or at least not exclusively. This approach works for Medicare, and it could work for schools also. What we really need is single-payer education – not single-provider education. Anyways, the point is that we think about these programs in somewhat inconsistent ways… Even people advocating single-payer want to be able to go to a private doctor. And yet, these same people are terrified of the government paying for education but not actively providing the schooling.
Kain is right that many school choice advocates want a single-payer, government voucher system. But he’s absolutely wrong to imply the libertarian preference is for a single-payer, government voucher system in education. [Note: I look at ideologies as structures reflecting what people think is valuable, what works and why in politics and society.]
In education, we begin with an almost fully socialized system unlike anything else in American society. So its no surprise that education reform discussions produce ideological confusion.
Vouchers, because they move the means of production out of the hands of the government, into the hands of private providers, and afford the consumer some decision-making powers, are improvements from a perspective that advantages individual liberty. But the single-payer, government funding, and regulation inherent in a voucher program remain massive defects from the libertarian perspective.
Our health care system is crippled by government regulation and single-payer (private employer and government) distortions. But it is not fully socialized or government-funded like our education system. A single-payer government health system would make matters worse from the libertarian perspective.
Think of these policy scenarios on a Left-to-Right ideological scale running from 1 on the far Left to 7 on the far Right, with 4 in the middle. Our standard government-financed, government-run, socialized education system is a 1, as far Left as one can go. Voucherizing the entire system would push it to a 2.
Kain is correct that “it’s a consistent position to support both single-payer healthcare … and single-payer education,” because both are completely and comfortably on the Left side of the policy spectrum. Vouchers can’t solve all of our problems in education policy.