
During the COVID-19 pandemic, Sweden stood out from other countries, stubbornly refusing lockdowns, school closures, and mask mandates. This was highly controversial and many outsiders saw it as a dangerous gamble with human lives. From a Swedish perspective, however, it looked like it was other countries that were engaging in a dangerous experiment.
This paper describes Sweden’s policies and the reasons for its choices, and it presents some preliminary conclusions about the results. Sweden’s economy got through the pandemic better than comparable countries, and elementary school students have not suffered learning losses. These benefits do not seem to have come at the expense of human health. Remarkably, total excess deaths were smaller in Sweden than in any other European country during the three pandemic years (2020–2022), and the rate was less than half of America’s. In the absence of strict government control, Swedes adapted their behavior voluntarily.
Introduction
Sweden was different during the pandemic, stubbornly staying open as other countries shut down borders, schools, restaurants, and workplaces. This choice created a massive interest in Sweden, and never before have the foreign media reported so much about the country. Many outsiders saw it as a reckless experiment with people’s lives. In April 2020 President Donald Trump declared that “Sweden is paying heavily for its decision not to lockdown.”1 In the New York Times, Sweden’s laissez faire approach was described as “the world’s cautionary tale” and in the same pages Sweden was described as a “pariah state.”2
There remains a popular perception in the rest of the world that Sweden’s strategy resulted in a human disaster, and many people think that Swedish decisionmakers came to regret the strategy and, in the end, adopted lockdown policies similar to those in other countries. This paper dispels those unwarranted assumptions, describes Sweden’s actual pandemic policy, explains why the country followed that course, and presents what we know about the results so far.
Sweden’s Strategy
The main difference between Sweden’s strategy, which was adopted under a government coalition of the Social Democrats and the Green Party, and that of most other countries, was that it mostly relied on voluntary adaptation rather than government force. The Corona Commission, an independent body formed by the government to evaluate the response, described it thus:
The approach chosen by Sweden was based on voluntary measures and personal responsibility, rather than more intrusive interventions … people have not been forced to the same extent as in many other countries to comply with regulations restricting their personal freedom.3
The government recommended that Swedes engage in social distancing, work remotely, avoid nonessential travel, and stay indoors if they felt sick, but it did not force them to. The Social Democratic Prime Minister Stefan Löfven declared: “We will never be able to legislate about everything. We will never be able to ban all harmful behavior. Now it is actually more a matter of common sense. There is an individual responsibility, and every individual has to take responsibility for themselves, for their fellow people and their country.”4 Those were concepts rarely heard in other countries at the time.
This does not mean that there were no restrictions in Sweden. The most restrictive was that public gathering and events were limited to no more than 50 participants in March 2020. This included theater, cinema, concerts, lectures, religious meetings, demonstrations, sporting events, and amusement parks, but not workplaces, shopping centers, and private gatherings. In November 2020 this limit was reduced to eight people, then gradually lifted starting in May 2021 until it was fully removed in September 2021.
In April 2020 the government banned private visits to elderly care homes. Bars and restaurants were ordered to offer table service only and the space between tables had to be increased. In November 2020, alcohol sales after 10 p.m. were banned, and by the end of the year, the deadline was advanced to 8 p.m. This rule was terminated in June 2021.
The Public Health Agency of Sweden recommended that secondary schools and universities switch to distance education between March and June 2020, and again in December 2020 until early January 2021, but preschools and elementary schools stayed open throughout that time.
Most countries, including Sweden’s neighbors Norway, Denmark, and Finland, rapidly closed their national borders. Finland even erected internal borders. Sweden’s state epidemiologist Anders Tegnell rejected border closures as being “ridiculous” and unscientific because the virus is already within a country that considers such a step, and restrictions would just hurt the economy.5 Still, when the European Union closed its borders to non-Europeans in March 2020, being a member of the EU, Sweden had to follow.
Featured Event
Despite these exceptions, Swedes experienced a very different pandemic. There was no state of emergency, no curfews, no orders to stay at home or shelter in place. Young Swedes were encouraged to continue with their sports training and events. Schools remained open, and so did offices, factories, restaurants, libraries, shopping centers, gyms, and hairdressers. As a rule, borders were not closed to fellow Europeans and public transportation kept running.
There were no mask mandates and not even a recommendation for the public to use masks—until January 2021, when they were recommended on public transportation during rush hours (7–9 a.m. and 4–6 p.m. on weekdays). While some other governments forced school children to wear face masks, Tegnell even warned against making children wear them, saying that “school is no optimal place for face masks.”6
One can see how Sweden’s path diverged from that of its peers by consulting the latest Human Freedom Index, which has data through 2020. During this first year of the pandemic, Sweden’s freedom rating only fell by 0.19 on a 10-point scale, compared to 0.49 in Britain and 0.52 in the United States. The only rich country that saw a smaller decline in freedom than Sweden was Singapore, at 0.16.7
Why Was Sweden Different?
The rest of the world wanted to know why Sweden chose to remain open. Swedes thought that the more pertinent question was: Why did other countries close down? In a span of just two weeks, 80 percent of the Organisation for Economic Co-operation and Development (OECD) countries adopted lockdown policies. What set Sweden apart was not some strange, unprecedented experiment, but the fact that Swedes did not suddenly and drastically change course. For decades the World Health Organization had planned for a pandemic, and lockdowns of entire societies were never part of the discussion. Instead, plans focused on protecting the most vulnerable but trying to keep society as a whole up and running. What set Sweden apart was that it stuck to that plan, and from a Swedish perspective, it looked like it was the rest of the world that was engaging in a risky, unprecedented experiment.8
A team of researchers tried to explain the timing of lockdown decisions in different countries by looking at the spread of the disease, the demographic structure, and the capacity of health care. They could not find any relationship except with one factor: what neighbors did. After China locked down and Italy followed suit, other countries that adopted lockdowns basically just copied each other.9
This is not science, but it makes political sense. If you follow the herd, and suffer on par with everybody else, then you can say that there was nothing much that could be done to have prevented that suffering. But if you act differently from everybody else and face abysmal results—worse than those of other countries—then you put yourself in a terrible position as a politician. This is why Sweden was such an irritation for other governments, and at times it seemed like some rooted for a Swedish disaster. The British health minister, conservative Matt Hancock, became so fed up with what he called the “f—–g Sweden argument” that he told one of his aides “Supply three or four bullet [points] of why Sweden is wrong.”10 Why—not if.
But the question remains: Why did Sweden not turn when everyone else turned? Several explanations have been suggested. Perhaps social distancing comes naturally to introverted Swedes, so that we don’t have to be compelled to engage in it. A joke that made the rounds was that “Finally no more 2‑meter rule, now Swedes can go back to the usual 5‑meter distance.” But fellow Scandinavian introverts in Denmark and Norway chose lockdowns (albeit not as prolonged as those in the rest of Europe and the United States).
Another explanation is that a society with a high level of social trust might rely on voluntary behavioral changes instead of resorting to mandatory ones. True, but again, other high-trust countries chose another path, and in fact, other populations began to engage in voluntary social distancing as soon as the pandemic started, before they were ordered to do so. One can also make the case that causation runs in reverse as well: it’s easier to follow general recommendations if you can make exceptions that are important to you. Governments that police people’s social life and enforce mask wearing might have problems retaining their residents’ loyalty and trust.
A third explanation is that the Swedish government does not have a constitutional right to lock down society and shut down businesses. But that just delays the policy, it does not rule it out. If parliament wanted to give the government such powers, it could, and this is exactly what was done with a temporary law in April 2020. Harsher policies were still seen as unnecessary and too intrusive, and almost none of these powers were used by the government.
There is some truth to all these explanations, but the most important reason was probably the unique division of power that Sweden has had since the 17th century. Governmental agencies are independent to an extent that they are not in other countries. The government appoints the directors-general of these agencies but does not tell them what to do. Instead, agencies are supposed to follow the law and the facts. Directors-general have set terms and are not replaced if the government changes after a general election. If the government thinks that someone has failed, it can replace that person, but this is a rare occurrence.
Traditionally, this has given agencies more freedom to stand clear of the electoral cycle and political agenda. It also gives ruling politicians an alibi: they can say that this is the advice they have been given by the experts and that they have no reason to challenge the experts. If the response to the pandemic would have turned out to be seriously wrong, the politicians could have blamed the expert agency and changed policy without losing face. This does not, of course, guarantee good advice. The world is full of expert agencies staffed by people obsessed with a single problem, who neglect trade-offs and ignore the cost of their decisions in terms of liberty and prosperity. However, by happy coincidences and specific historical circumstances, Sweden’s public health agency had other kinds of people in charge.11
During the pandemic, this independence helped the agency chart a more liberal course. In some other countries, public health authorities thought more along the Swedish lines but were overruled by politicians who faced a demand to show strength. For example, the Danish and Norwegian agencies were opposed to closing borders and schools, but political considerations trumped their concerns. Even in Britain, where the popular perception is that the government eventually agreed to a lockdown because scientific advisers called for it, it has been revealed that Prime Minister Boris Johnson’s powerful political adviser Dominic Cummings pressed the government’s independent scientific advisers to recommend faster and broader lockdown measures.12
In Sweden, where there was less need for political grandstanding, the public health agency guided policy and politicians felt comfortable not overruling the agency. Its arguments were twofold: first, you can’t focus all your efforts on a single problem, and second, recommendations are more sustainable than government control. There are important considerations that could be threatened by a lockdown: the loss of learning, community, production, and livelihood. People don’t just suffer from viruses, they also suffer from loneliness, mental illness, domestic abuse, unemployment, and other effects of stringent lockdowns. People can’t live under a lockdown forever, and therefore they will begin to suffer and eventually break the rules, and when that happens the virus will break through. Countries that shut down will not avoid deaths, but just delay them, at a high social and economic cost. Since it was not known when a vaccine would be available, or how effective it would be, it was important to come up with ways of living that could be sustained for a long time.
In a Nature interview in April 2020, Sweden’s state epidemiologist Anders Tegnell, the public face of Sweden’s strategy, said: “Closedown, lockdown, closing borders—nothing has a historical scientific basis, in my view. We have looked at a number of European Union countries to see whether they have published any analysis of the effects of these measures before they were started and we saw almost none.”13
What Did Swedes Think?
This policy choice was controversial, but it was mostly supported by the population. The share of Swedes saying that they approved of their government’s COVID-19 strategy was 53 percent in June 2020; it fluctuated between 42 and 62 percent throughout the pandemic and in January 2022 it was back at almost exactly the starting point, at 52 percent. That is more than twice as many as were critical of the strategy—23 percent. The share that thought that too little consideration was being taken of public health was 17 percent in March/April 2020. In January 2022, it was still 17 percent.14
Polls in March and April 2020 showed that more than 70 percent of Swedes trusted the public health agency and in January 2022, 68 percent did.15 Fifty-three percent said that they had trust in state epidemiologist Anders Tegnell in March 2020, making him more popular than any of the leaders of the political parties. This increased to almost 70 percent in May but fell to 54 percent in January 2021. However, this amounts to a high net approval of Tegnell, as no more than 22 percent expressed little trust in him.16
Support for the governing Social Democratic party grew. In early 2020 the party stood at around 23 percent in the polls, but as the virus surged, support for the party increased to more than 30 percent. This was partly a “rally round the flag” effect, and the numbers declined slightly later on, but the party still achieved a 30.3 percent vote share in the September 2022 election, beating the expectations.
Featured Event
The relative popularity of Sweden’s approach was reflected in the fact that opposition parties did not see an electoral advantage in attacking it. The center-right parties basically called a political truce and rarely challenged the government’s overarching strategy. The one major exception was the nationalist populist Sweden Democrats, which called for a closure of Sweden’s schools and for Tegnell’s removal as state epidemiologist. The party declined in the polls, from around 25 to 20 percent, and as the popular backlash against the strategy failed to arrive, the Sweden Democrats grew more silent in their opposition rather than doubling down.
A popular perception has taken hold in other countries that Swedish decisionmakers came to regret the country’s strategy as fatalities mounted, so they apologized and backtracked. The most important source for this interpretation is a misunderstanding of an interview with Anders Tegnell on Swedish public radio in June 2020. Tegnell replied to a question by saying that, in retrospect, Sweden would have done some things differently if it had had all knowledge in advance. This was widely reported around the world as a statement of remorse and an abandonment of the openness strategy. For example, the Telegraph headlined it as “Architect of Sweden’s Coronavirus Strategy Regrets Not Imposing Tougher Lockdown,” and the Washington Post reported “Scientist Behind Sweden’s COVID-19 Strategy Suggests It Allowed Too Many Deaths.”17
Tegnell however, denied that interpretation: “It’s not like that at all, we still think the strategy is good, but there are always improvements you can make, especially when you have the benefit of hindsight. And personally I think it would be quite strange if you answered such a question differently.”18
When asked about what specific improvements he had in mind during a press conference the same day, Tegnell answered that Sweden should have done more to protect nursing homes and to scale up testing capacity.
Similar exaggerated and outright false interpretations ensued when Sweden’s king and prime minister talked about the loss of lives as a “failure” and said that nursing homes should have been better protected. The BBC described this as “Swedish King Carl XVI Gustaf Says Coronavirus Approach ‘Has Failed,’” and Bloomberg as “Swedish Prime Minister Admits Strategy to Stop Virus Fell Short.”19 Neither the king nor the prime minister ever described the overall strategy as mistaken or suggested that Sweden should have been locked down.
How Did It Turn Out?
Analysts from other countries—and even some Swedish scholars—predicted disaster. One influential Swedish model, inspired by the famous British Imperial College study, predicted that Sweden would have 20,000 COVID-19 patients needing intensive care by early May 2020 and a need for intensive care units around 40 times over capacity. By July 1, Sweden would have 82,000 COVID-19 deaths.20 The Imperial College model predicted between 66,000 and 90,000 deaths without mitigation efforts, and a peak demand of intensive care unit patients 70 times higher than capacity.21
Sweden’s public health agency planned for a worst-case scenario that was much less pessimistic, suggesting a peak of around 1,700 intensive care patients in the middle of May. Still, that was more than three times the pre-pandemic capacity in health care.
Sweden did suffer quickly and on a large scale. Swedish children have an annual weeklong winter break, during which many Swedish families go to the Italian and Austrian Alps for skiing. In 2020, Stockholm schools had this break from February 17 to February 23, at the same time that infections surged in northern Italy, so Stockholm families imported the virus on a large scale before it was considered a major concern and before lockdowns were even discussed in other Western countries. The importance of this timing is revealed by the fact that infections did not surge in Sweden’s second- and third-largest cities, Gothenburg and Malmö, which had their winter break in the two preceding weeks.
But eventually the virus spread rapidly through the population. At times during the spring of 2020 Sweden had some of the highest COVID-19 death rates in Europe. The infection made its way to many residential care facilities for the old. As the Corona Commission would later conclude, the ambition to protect such high-risk groups was “an approach that emerged fairly quickly as more of a hope than a plan of action.”22
By July 1, 2020, Sweden had experienced 517 COVID-19 deaths per million people, which was lower than Italy and Spain but as much as 5 to 10 times higher than its geographically and culturally closest neighbors, Norway, Denmark, and Finland. This made Sweden’s approach to COVID-19 look like a fiasco.23
That summer, the New York Times described Sweden as a “pariah state” and a “cautionary tale.”24 Reuters reported: “Sweden’s Liberal Pandemic Strategy Questioned as Stockholm Death Toll Mounts”25 and President Donald Trump dismissed the strategy out of hand: “Now, they talk about Sweden, but Sweden is suffering very greatly. You know that, right? Sweden did that. The herd. They call it the herd. Sweden is suffering very, very badly.”26
But even this early in the pandemic it was obvious that the dire projections by Swedish and other modelers were far off the mark. By early July, Sweden had not suffered the 82,000 deaths that the models had assumed, but 5,455—less than 7 percent of what was predicted. And evidence suggests that those people did not die because the health care system was overwhelmed. Even during the peak, when models had expected 40 to 70 people to fight over every hospital bed, there was an excess capacity of intensive care units of around 20 percent. In Stockholm, a new field hospital was built to house hundreds of patients, but journalists were left outside waiting for the first patients to arrive in vain. It was dismantled before it even had to open.
An argument can be made that media amplification of the models’ dark projections scared Swedes into changing their behavior and ramping up health care capacity, and so helped to avoid a disaster. But in fact, most of the models had assumed that it was already too late, even if Sweden switched to strong mitigation. The need for intensive care unit beds in Sweden will be “at least 10-fold greater if strategies approximating the most stringent in Europe are introduced by 10 April” (which of course they weren’t), wrote Uppsala University’s Jasmine M. Gardner and her colleagues, for example.27
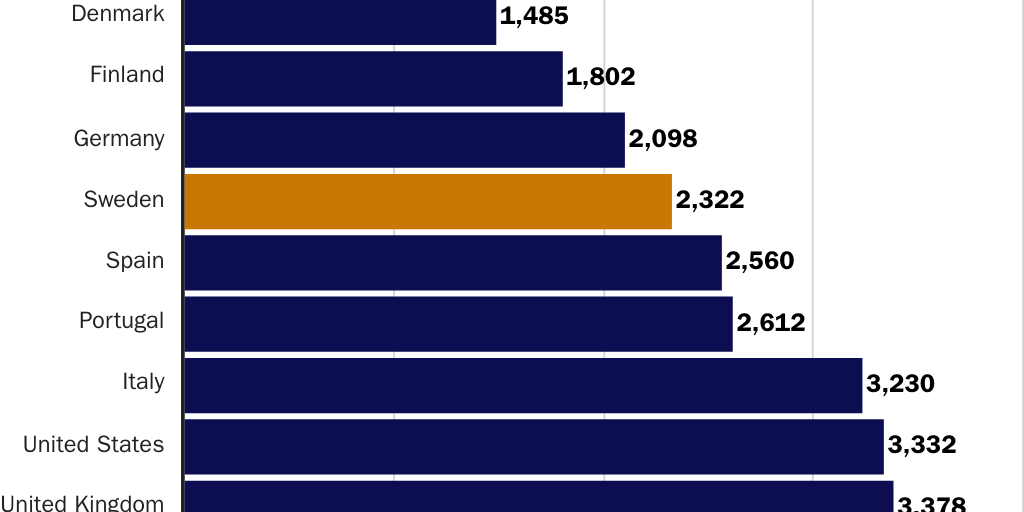
By June 14, 2023, Sweden had suffered a total of 2,322 COVID-19 deaths per million people. That was still almost 40 percent higher than Norway, Denmark, and Finland, but nowhere near 5 to 10 times their death rates as in the beginning of the pandemic. And it is a lower rate than that of Southern Europe—and much lower than the United States and the United Kingdom, which both had more than 3,300 deaths per million people (see Figure 1).28
Despite the rapid invention and global rollout of a vaccine, contrary to the expectations of the Swedish public health agency, it was proven correct that Sweden’s comparatively dismal performance at the start of the pandemic was mostly a result of other countries having managed to delay cases and deaths, rather than having prevented them. Sweden suffered most of its deaths in 2020, while the Nordic neighbors and many other countries got them in 2022.
Excess Deaths
However, the number of COVID-19 deaths is not as simple a statistic as it seems. Some countries did not count deaths outside hospitals. When patients died at home or in nursing homes they were not automatically included in the data sets. In Sweden, by contrast, authorities automatically checked the lists of people who were infected against the population register, so everyone who died and had tested positive for the virus was counted as a COVID-19 death, even if they died from a heart attack or a fall. So in effect, Sweden reported many who died with COVID-19, not of COVID-19.
Even in a country as similar to Sweden as Norway, deaths were counted as a COVID-19 death only if the attending physician concluded that COVID-19 was the cause of death and called the country’s public health agency to report it. “It is possible that Norway could have a higher number of registered deaths if we counted as Sweden,” said a doctor at Norway’s public health agency in April 2020.29
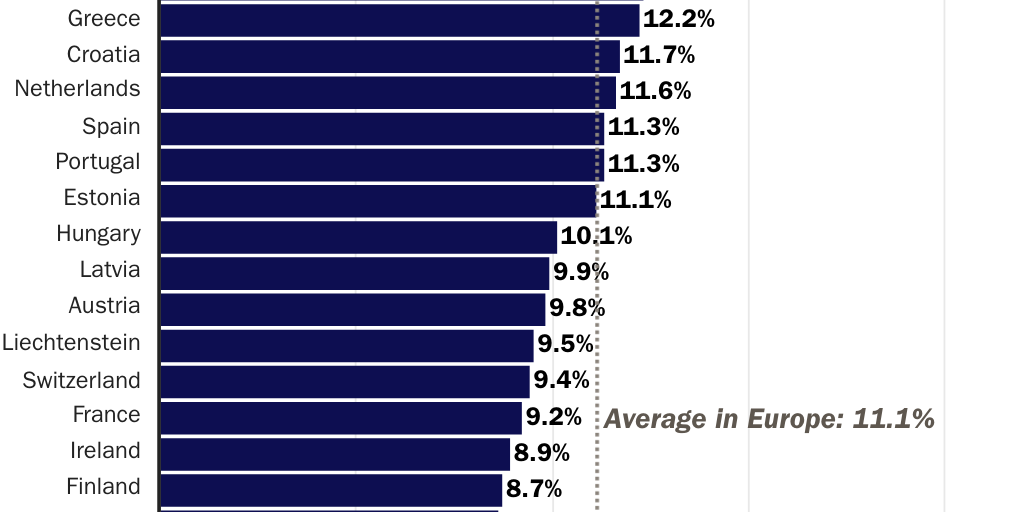
This is why so many scholars and decisionmakers insisted that it was necessary to wait for a broader perspective and look at excess deaths, that is, the number of deaths over a period compared to a previous period or an expected value. Now we have those numbers. When you look at excess deaths during the three pandemic years, 2020–2022, compared to the previous three years, you get a very different picture. According to this measure, Sweden’s excess death rate during the pandemic was 4.4 percent higher than previously. Compared to the data that other countries report to Eurostat, this is less than half of the average European level of 11.1 percent, and remarkably, it is the lowest excess mortality rate during the pandemic of all European countries, including Norway, Denmark, and Finland (see Figure 2).30
These numbers, though surprising, are not controversial. These are the numbers that each country reports for themselves. The crude excess death rate, however, is a blunt measure. It does not take into consideration the population structure, such as age and health. It treats deaths from COVID-19 just as it does deaths from traffic accidents and suicides. Yet it is a way of getting around the problem that countries count COVID-19 deaths differently, and it is an important corrective to the assumption that Sweden willingly sacrificed lives on a massive scale.
The numbers can be adjusted for what was to be expected from population predictions, even though such data does not exist for all countries, and the choice of method leads to varying results. When Statistics Sweden compares excess deaths with projected deaths based on population trends and age, at 4.2 percent Sweden still has fewer excess deaths than its neighbors, but the difference with Denmark (4.3) and Norway (4.5) becomes insignificant. Finland’s rate is almost twice as high, at 8.2 percent.31
The result is slightly different when the website Our World in Data uses the Human Mortality Dataset and compares excess deaths with the previous five years rather than the previous three years. Then Denmark has a lower rate than Sweden, with Norway close to Sweden and Finland higher than Sweden.32The Economist has its own method for measuring excess death and comes to a similar conclusion.33
Despite differences in methods and results, all these studies suggest that in terms of COVID-19 fatalities, Sweden is a typical Nordic country. That is startling, since in comparison with its neighbors, Sweden has higher population density, more overcrowded households, and a higher share of foreign-born people (a group that turned out to be particularly vulnerable). Preben Aavitsland at Norway’s public health agency concludes that “other countries managed to delay some deaths, but now, three years after, we end up at around the same place.”34 Just as Sweden’s epidemiologists had predicted.
And of course, the Nordic region did very well in an international comparison. According to Our World in Data, Sweden’s excess death rate was 5.6 percent compared to 10 percent in Britain and 14 percent in the United States. With The Economist’s method, Sweden’s excess death rate was around 180 per 100,000 people, compared to 345 in Britain and 400 in the United States.
After all was said and done, astonishingly, Sweden had one of the lowest excess death rates of all European countries, and less than half that of the United States.
One reason why Sweden got through the pandemic in a much better shape than many scholars, journalists, and politicians expected was that they only thought in terms of strict government controls or business as usual. They failed to consider a third option: that people adapt voluntarily when they realize that lives are at stake. Swedes quickly changed their behavior and mostly followed the recommendations. As early as April 2020, half the workforce worked from home and public transport usage had declined by half. Mobility data from telecom providers show that mobility patterns in Sweden were similar to those in neighboring countries. If anything, Swedes reduced their travel a bit more in the aggregate.35
The difference was that if Swedes decided, based on local knowledge and individual needs, that they had to go to work, exercise, or meet a relative or a friend, they could do that without being stopped by the police. This meant that the pandemic became less politicized in Sweden and perhaps also that people accepted the need to live under extraordinary conditions for longer than they would have if they didn’t have these individual emergency exits.
Other Indicators
The Swedish economy is very open and export dependent, so when the world suffers, so does Sweden. However, Sweden’s economy did much better than comparable countries. The world economy was 2.9 percent smaller after 2021 than it would have been according to the Organisation for Economic Co-operation and Development forecast before the pandemic; the Eurozone 2.1 was percent smaller, and the U.S. economy 1.2 percent smaller. The Swedish economy was 0.4 percent bigger.36 This is even more exceptional since the Swedish government introduced much less fiscal stimulus than most other countries.
Of more importance for the future is the learning loss in countries where children were not allowed to go to school for months, and, in some cases, years. An international study in Nature Human Behaviour finds that on average, students lost out on more than a third of a normal school year’s worth of learning. Most worrying, those closures hit poorer families harder, as they could not compensate from school closures in the way socioeconomically advantaged families could.37
The U.S. Department of Education concluded that half of America’s students began 2023 a full year behind grade level in at least one subject. “We’re seeing that they’re starting the school year off about the same as they were last year,” says Rachel Hansen at the National Center for Education Statistics.38
In sharp contrast, Swedish elementary schoolers suffered no learning loss during the pandemic, according to a study in the International Journal of Educational Research that examined word decoding and reading comprehension. The scores were not lower during the pandemic and children from low socioeconomic backgrounds were not especially affected.39
In lockdown countries, other health interventions suffered when all action was focused on COVID-19. In 2021 alone, 25 million children missed out on childhood vaccinations globally, the biggest drop in 30 years.40 In some American states there was a drop in coverage with measles, mumps, and rubella vaccines of around 5 percentage points during the pandemic.41 By contrast, Sweden did not suffer a drop at all. In 2020 the Swedish childhood vaccination rate was 97.2—up by a tenth of a percentage point from the year before.42
Fear and isolation during the pandemic may have affected mental health and increased feelings of loneliness and depression. However, most studies only cover the beginning of the pandemic, and it will take time until we know about the long-term effects on mental health. A review of general population studies up until April 2022 showed small overall changes for mental health during the pandemic but raised the possibility that vulnerable groups may experience issues that differ from the rest of the population.43
According to the World Happiness Report, self-reported well-being did not decline in Sweden during the pandemic. However, this is less exceptional than it sounds, since the global average was also just as high in 2020 to 2022 as it was in 2017 to 2019. Overall life evaluations seem resilient, even though, again, averages can hide drops for smaller, vulnerable groups.44
Sometimes in the midst of a major disaster there are fewer suicides, but as the effects of post-traumatic stress disorders play out, there are more of them. This seems to have been the case during the pandemic as well. In the initial months many countries reported fewer suicides, but a 2022 review of 1,052 studies of suicide found that a majority of studies reported an increasing trend in the number of suicides during the pandemic.45 In Sweden, there was no increase in suicides, but rather a small decrease from 2019 to 2021.46
As couples under stay-at-home orders were forced to remain under the same roof, instances of domestic abuse increased. A study of the United States and six other countries concluded that lockdowns increased domestic abuse by around 8 percent.47 The same method has not been used to analyze Sweden’s situation, but the reported number of cases of abuse against women and girls by a present or former partner declined by around 25 percent between 2020 and 2022.48
We should be careful with these data since they are preliminary; international comparisons are difficult and the long-term effects of lockdowns are still unknown. However, they all indicate that Sweden did much better than other countries during the pandemic.
Conclusion
The independent Swedish Corona Commission, formed by the government after pressure from parliament, was critical of many aspects of how authorities acted during the pandemic, but the overall conclusion was positive:
The choice of path in terms of disease prevention and control, focusing on advice and recommendations which people were expected to follow voluntarily, was fundamentally correct. It meant that citizens retained more of their personal freedom than in many other countries … [and] many countries that have pursued [another] approach have experienced significantly worse outcomes than Sweden, indicating at present, at least, that it is highly uncertain what effect lockdowns have in fact had.49
When choices were made about pandemic strategies, the end result could not be known, and yet many politicians and journalists in countries including the United States, Britain, and Norway attacked Sweden fiercely for choosing an unusual and more liberal path. Why was that? Preben Aavitsland, Norway’s state epidemiologist, has recently come up with an explanation:
I think it may be because everyone was unsure of what was the right response to the pandemic. And yet, almost everyone at the same time chose to do long, hard lockdowns early on, inspired by Italy which in turn was inspired by the communist dictatorship China.
Sweden became the contrast they did not want. Sweden undermined their mantra that we had no choice and forced them to explain to their citizens why they did what they did. For these colleagues, it would have been better if everyone had done the same. They hid their own insecurities by lambasting Sweden.50
Now we know more. It seems likely that Sweden did much better than other countries in terms of the economy, education, mental health, and domestic abuse, and still came away from the pandemic with fewer excess deaths than in almost any other European country, and less than half that of the United States—the country where both the president and major newspapers repeatedly used Sweden as a cautionary tale. The conclusion is uncomfortable for other governments. It was not Sweden that engaged in a reckless, unprecedented pandemic experiment, but the rest of the world. This experiment did not turn out well compared to the one country that did not throw out the manual. Millions of people were deprived of their freedoms without a discernible benefit to public health.
This is a lesson for the next disaster—whatever it is, and whenever it strikes. Harsh pandemic restrictions were often defended with reference to the precautionary principle—do not take a particular course of action before an abundance of evidence is available. But there was no evidence indicating that drastic restrictions made sense. In times of uncertainty it doesn’t seem like a precaution to put all your policy eggs in one basket and add to the burden of a health emergency by undermining communities, the economy, and education. Instead, it seems like negligence. Sweden’s alternative model was to rely more on recommendations, have faith in voluntary adaptations to the pandemic, and try to keep as much of society up and running as possible. Based on what we now know, this laissez faire approach seems to have paid off.
Citation
Norberg, Johan. “Sweden during the Pandemic: Pariah or Paragon?,” Policy Analysis no. 959, Cato Institute, Washington, DC, August 29, 2023.

About the Author


This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.