
Every state except Alaska has laws that criminalize the possession and/or sale of paraphernalia for the consumption of illicit drugs. State-level drug paraphernalia laws prevent people who use those drugs from accessing the means to reduce the risk of infection or overdose. This makes nonmedical drug use even more dangerous because the laws often prevent access to clean needles and syringes along with products to test drugs for deadly contaminants.
These laws are meant to discourage illicit drug use. Instead, they produce avoidable disease and death. Drug prohibition puts peaceful, voluntary drug users at risk of losing their liberty and often their lives. Paraphernalia laws similarly increase the risk that users will lose their lives.
Some states have amended their laws to permit harm-reduction programs and tools. For example, many states allow syringe services programs (also called SSPs or “needle exchange programs”) to operate within narrowly defined parameters.
The goal of drug paraphernalia policy should be to save lives by reducing the risks of overdose and disease. This means removing government barriers to obtaining and distributing clean syringes and drug testing equipment. Because Alaska leaves residents free to purchase syringes and other paraphernalia in any quantity, anyone can operate an SSP and implement other harm-reduction measures. States should follow Alaska’s lead by repealing their drug paraphernalia laws so that programs aimed at reducing overdoses and disease can proliferate and succeed.
Introduction
State-level drug paraphernalia laws prevent individuals from protecting themselves against many of the risks of using drugs obtained on the black market. Some paraphernalia laws deny drug users access to fentanyl test strips, a vital means of screening drugs for contamination with the dangerous opioid responsible for the great majority of opioid-related overdose deaths.1 Several studies have found that if nonmedical drug users have access to fentanyl test strips, they are likely to use them to alter their drug use behavior, “including discarding their drug supply, using with someone else, and keep[ing] [the opioid overdose antidote] naloxone nearby.”2 Also, some paraphernalia laws restrict people from purchasing or possessing clean needles and syringes, increasing the risk of infection from sharing and reusing those items.
Drug paraphernalia laws also threaten to punish nonusers involved in harm reduction. People risk incarceration if they give out or obtain clean needles and syringes, test strips to check for dangerous additives or contaminants in drugs obtained on the black market, or materials to clean drug use equipment. Paraphernalia laws prevent governmental and nongovernmental organizations from creating syringe services programs (SSPs), also known as needle exchange programs.3 SSPs reduce the spread of HIV, hepatitis, other blood-borne infectious diseases, and soft tissue infections. More recently, they have proven helpful in reducing drug overdoses.4
Federal law does not interfere with states operating or permitting privately run SSPs. However, many state drug paraphernalia laws prohibit these services. Some states carve out exceptions for SSPs in their drug paraphernalia laws, yet these exceptions often include restrictions on the number of SSPs allowed, restrictions on the entities that may operate them, and onerous conditions they must meet.5 These impede the development and proliferation of SSPs.
Lawmakers and policymakers from across the political spectrum are increasingly recognizing and embracing harm-reduction strategies to reduce death and disease from illicit substance use.6 Yet drug paraphernalia laws stand in the way of harm reduction, including harms that drug prohibition itself causes.7 This paper examines which states most allow drug users to take precautions to reduce the risks of drug use and drug prohibition.
Drug Paraphernalia Laws and Harm Reduction
Federal and state laws prohibit or severely restrict access to equipment that can help people use drugs more safely. Federal laws prohibit transporting drug paraphernalia across state lines, whereas state laws focus on intrastate trafficking. Federal and state statutes vary in how and what they define as paraphernalia. Both federal and state paraphernalia laws obstruct private harm-reduction organizations that seek to save lives, but state paraphernalia laws have a more direct and deleterious effect on harm reduction.
Drug Paraphernalia Laws
Under the federal drug paraphernalia statute of the Controlled Substances Act, it is illegal to sell, transport through the mail, import, export, or transport across state lines “any equipment, product or material of any kind which is primarily intended or designed for use in manufacturing, compounding, converting, concealing, producing, processing, preparing, injecting, ingesting, inhaling, or otherwise introducing into the human body a controlled substance.” Examples include pill presses, drug testing kits, test strips, glass and metal pipes used to smoke crack cocaine and methamphetamine, specialized glass products, scales, cone-shaped marijuana/hash pipes called “chillums,” and even miniature spoons.8
States vary in what they define as drug paraphernalia. For example, Arizona prohibits possession, “with intent to use, drug paraphernalia to plant, propagate, cultivate, grow, harvest, manufacture, compound, convert, produce, process, prepare, test, analyze, pack, repack, store, contain, conceal, inject, ingest, inhale or otherwise introduce into the human body a drug in violation of this chapter.”9 Illinois law specifies as prohibited paraphernalia “testing equipment intended to be used unlawfully in a private home for identifying or in analyzing the strength, effectiveness, or purity of controlled substances.”10
Simple possession of drug paraphernalia is not a federal crime. However, some state laws prohibit owning or possessing these items. In some instances, local police may check a pipe, hookah, or bong for residue. If they determine the possessor uses it to ingest an illicit substance, they may press charges against that individual. If they determine it was acquired legally for a legal purpose (e.g., a syringe to inject insulin for diabetes), they will let them keep it. Unfortunately, many types of drug paraphernalia that states restrict or prohibit are also important harm-reduction tools.
Fentanyl Test Strips, Harm Reduction, and Paraphernalia Laws
Fentanyl test strips save lives by enabling drug users to detect the presence of this dangerous opioid in other drugs, such as heroin and cocaine.11 Researchers claim the tests strips are highly accurate and can detect up to 10 analogs of fentanyl, such as 2‑flourofentanyl and crotonylfentanyl.12 Users who detect fentanyl typically discard the contaminated drugs, use smaller amounts, and/or take the drug more slowly, thereby reducing the risk of overdose.13
Many states prohibit fentanyl test strips as paraphernalia because individuals use them to test or analyze an illicit drug. As a result, people end up overdosing because the ban prevents them from determining what would be a nonlethal dose.
Some states are beginning to correct this deadly mistake. In May 2021, Arizona amended its drug paraphernalia law to exclude fentanyl test strips from its definition of paraphernalia.14 Pennsylvania’s attorney general and Philadelphia’s district attorney announced that they will not prosecute people arrested for possessing fentanyl test strips, which are illegal in the state. Philadelphia Mayor Jim Kenney issued an executive order telling police to not arrest people who possess fentanyl test strips.15
SSPs, Harm Reduction, and Paraphernalia Laws
Decades of evidence on SSPs show that they reduce drug overdoses and the spread of HIV, hepatitis, and other blood-borne infectious diseases. They also promote and facilitate treatment and rehabilitation of participants who suffer from substance use disorder.16 These programs distribute clean needles and syringes to intravenous (IV) drug users. Many programs also distribute fentanyl test strips along with bleach and other materials to clean syringes and needles. Some offer HIV and hepatitis blood tests and refer for treatment those who test positive.
Featured Video
The first such program arose in the Netherlands in the 1970s in response to an outbreak of hepatitis B. The idea gained acceptance in other countries with the advent of the AIDS pandemic. Congress banned federal funding of SSPs in 1988 in response to concerns that they encourage or enable IV drug use. In the hope that SSPs would mitigate the rise in HIV and hepatitis cases among IV drug users, Congress lifted the ban in 2015.17 The oldest continuous SSP in the United States started operating in Tacoma, Washington, in 1988.18 By the end of 2018, SSPs were operating in 39 states plus the District of Columbia and Puerto Rico.19 In many states, SSPs are in community health clinics that also offer referral for addiction therapy and counseling. To increase outreach, some programs operate mobile vans or delivery services or have centers along pedestrian routes.20 In recent years, SSPs have been distributing free kits of naloxone, the antidote to opioid overdose.21
Seven federally funded studies conducted between 1991 and 1997 found that SSPs reduce the risk of HIV infections among intravenous drug users and their partners.22 A 2013 systematic review conducted by the U.S. Centers for Disease Control and Prevention (CDC) confirmed that SSPs decrease the prevalence of HIV and hepatitis C infections.23 A 2014 systematic review and meta-analysis of 12 studies comprising 12,000 person-years found that SSPs coincided with a 34 percent reduction in the rate of HIV transmission, including a 58 percent reduction among the six studies that were rated “higher quality” on the Newcastle–Ottawa Scale.24
The CDC endorses and promotes SSPs with guidance and, in some cases, provides financial assistance for these facilities to local jurisdictions.25 The World Health Organization, the American Medical Association, the American Public Health Association, the American Society of Addiction Medicine, and the American Psychiatric Association all support and encourage SSPs. The Substance Abuse and Mental Health Services Administration and the National Academies of Sciences, Engineering, and Medicine endorse SSPs. Former U.S. surgeon general Jerome Adams, who served during the Trump administration, gave many public presentations in support of SSPs.26
Local law enforcement community members increasingly recognize that these programs can decrease the spread of communicable and infectious disease as well as protect first responders from accidental injury from contaminated needles.27 On December 7, 2021, the Substance Abuse and Mental Health Services Administration announced a new $30 million grant program to aid community-based harm-reduction programs, including SSPs.28 With the announcement, the White House’s Office of National Drug Control Policy released the Model Syringe Services Program Act to assist state lawmakers seeking to expand the availability of SSPs.29 The model legislation would eliminate many state restrictions that reduce SSP efficacy.
Despite this broad support and convincing evidence, many states inhibit the private sector from creating SSPs.30 In a 2009 national survey, a significant number of programs reported that police confiscate syringes and even arrest clients on their way to and from syringe services centers. Confiscation and arrests occurred more than four times more frequently in areas where SSP clients were predominantly people of color.31
While some SSPs receive government funding, many do not. The Grand Rapids Red Project (Michigan), Challenges Inc. (South Carolina), and Shot in the Dark (Arizona) are examples of successful and long-standing SSPs that operate solely with private funds.32 Voluntary private funding has advantages over government. Many object to government funding on the grounds that their tax dollars might enable illicit substance use and for other reasons. Such groups use the political process to impose funding conditions that limit SSPs’ effectiveness and to demand cuts that imperil their sustainability. After needle-sharing by IV drug users caused Scott County, Indiana, to suffer an HIV outbreak in 2015, for example, then governor Mike Pence authorized the state to create Indiana’s first SSP as an emergency measure. Health officials credited the program with a dramatic drop in the number of HIV cases. In 2021, however, Scott County commissioners voted to end the program. According to one report, commissioners who voted to end the program “say they can’t live with a program that makes it easier to abuse drugs.”33 By contrast, SSPs that receive only private funds have more stability and flexibility to develop innovative ways to protect drug users without imposing a cost on taxpayers.
Critics view SSPs as flouting the law, express discomfort with what they see as government sanctioning of intravenous drug use and other illegal activities, and argue that these sites do little to deter illegal drug use. They also claim that even if SSPs save lives, taxpayers should not finance them in a system of limited government—especially if private groups are willing to organize SSPs. (Presumably, these critics likewise oppose limited government prosecuting the operators of these private SSPs.) Supporters, on the other hand, claim SSPs not only save lives but also public funds by reducing the spread of communicable and infectious diseases.
The empirical evidence shows that SSPs save lives by reducing the spread of deadly and infectious diseases without increasing illicit drug use or crime.34 Furthermore, SSPs reduce disease among intravenous drug users’ intimate contacts who are not engaging in illicit drug use. SSPs also might possibly reduce disease spread to first responders. With the advent of state laws facilitating the wider distribution of fentanyl test strips and naloxone, studies suggest that SSPs might reduce overdose deaths as well.35
Comparing State Paraphernalia Laws
The 50 states and the District of Columbia have diverse drug paraphernalia policies. They differ on how they define drug paraphernalia and what they ban. Some state paraphernalia laws are more detailed.
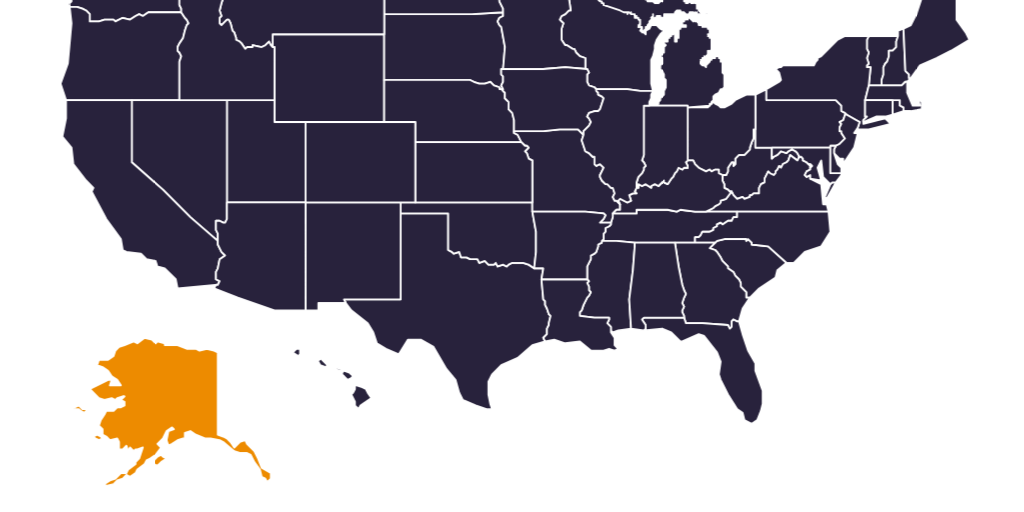
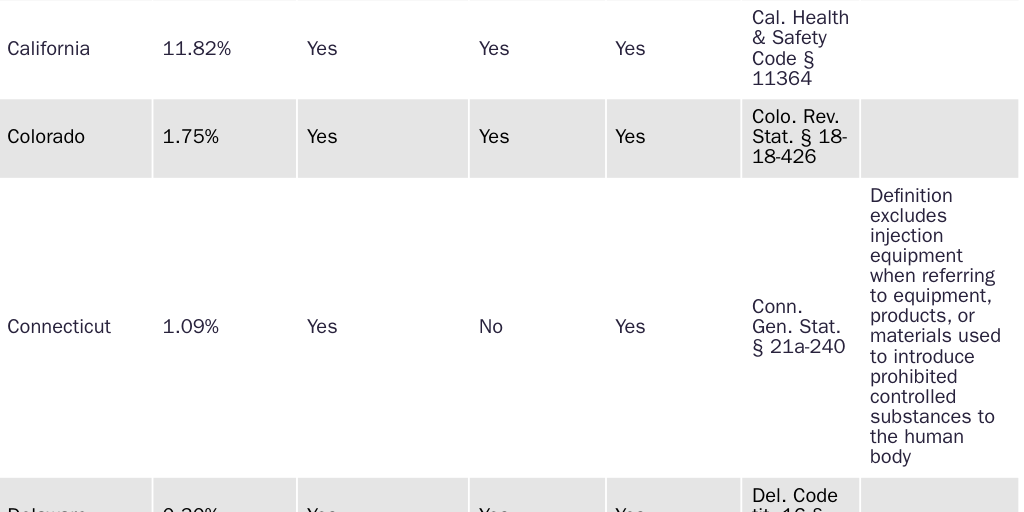
Alaska has no laws restricting drug paraphernalia, which leaves residents with maximum freedom to design syringe exchange programs and other harm-reduction initiatives. Of the other 49 states and the District of Columbia, 40 define drug paraphernalia to include syringes and 45 include testing materials. Thirty-five states and the District of Columbia limit both syringes and testing equipment. Four states limit syringes but not testing materials, whereas nine states limit purity testing equipment but not syringes. Only South Carolina excludes both syringes and testing materials from its definitions of drug paraphernalia, allowing SSPs to operate without restrictions. While South Carolinian law restricts the sale of needles and syringes, the law doesn’t affect SSPs, which give needles and syringes away rather than sell them.36 Montana prohibits both syringes and fentanyl test strips as illegal paraphernalia yet specifically exempts SSPs from the ban.37 Virginia places even more obstacles in the way of harm reduction by barring syringes and fentanyl test strips as illegal paraphernalia. While the state exempts employees and clients of SSPs from the ban, the Virginia health commissioner must approve all SSP operators.38 (See Appendix A.)
State Paraphernalia Laws
State definitions of paraphernalia commonly include kits to develop, grow, or otherwise manufacture controlled substances; blenders, bowls, and mixing devices that compound controlled substances; scales and balances that weigh or measure controlled substances; and various vaguely defined items that can potentially facilitate illicit drug use. Instructions on how to determine whether an item qualifies as drug paraphernalia often accompany these statutory definitions. These instructions become necessary because many of the listed items have legal uses. Some states, like Florida, include among the list of potential paraphernalia commonplace objects, such as two-liter soda bottles and duct tape.
States that explicitly authorize SSPs make exceptions to the definitions of paraphernalia to exclude syringes and other items if SSPs provide them. Other states remove syringes from the definition entirely, and still others specifically remove fentanyl test strips from the definition. These exceptions and workarounds can be confusing.
Figure 1 compares the 50 states and the District of Columbia with respect to drug paraphernalia laws and whether the definition of drug paraphernalia includes syringes and/or fentanyl test strips. Most states do not specifically cite fentanyl test strips but rather include as paraphernalia any materials that can test the purity of controlled substances. Appendix A provides more detail.
Public Access to Needles and Syringes
Needles and syringes are necessary to treat several routine medical conditions, such as injecting insulin to treat diabetes. People can legally obtain needles and syringes through pharmacies, though some states require prescriptions. Other states let people buy syringes only on a “behind the counter” basis (i.e., by asking a pharmacist or a pharmacist’s assistant or technician, rather than off the shelf). State policies differ regarding public access to needles and syringes independent of their SSP policies. Figure 2 shows the states that require a prescription to purchase syringes. Appendix B compares how easy it is for people in the 50 states and the District of Columbia to purchase needles and syringes.
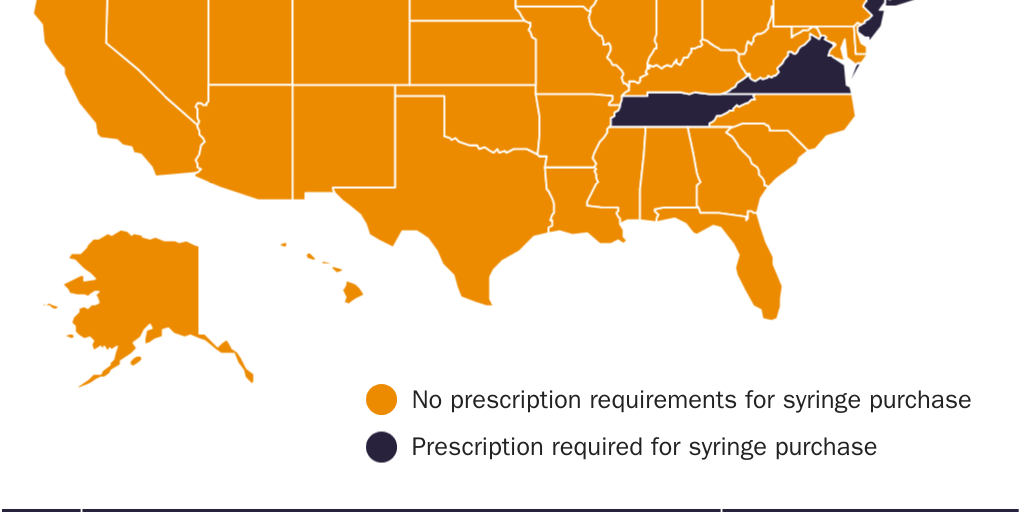
Drug paraphernalia laws often burden patients who need needles and syringes for medical use. Four states—Connecticut, Minnesota, New Jersey, and New York—require a medical prescription to purchase more than 10 syringes at a time. Tennessee and Virginia require consumers to provide pharmacists proof of medical need. Kentucky requires customers to offer a reason for the purchase and how they intend to use the syringes before a pharmacist may sell them. Such restrictions limiting the availability of sterile syringes increase intravenous drug users’ risk of blood-borne infectious diseases. When government blocks access to new (sterile) hypodermic needles and syringes, people end up reusing and sharing old needles and syringes. This practice leads to the transmission of HIV, hepatitis C, and other diseases.
Syringe access restrictions also burden pharmacists. Georgia, Ohio, Oklahoma, and Washington threaten pharmacists with fines and/or misdemeanor charges unless they can establish that they had a “reasonable expectation” that purchasers will use syringes for legal purposes. Such laws discourage syringe sales.39 One study found such regulations caused pharmacists to be less willing to sell syringes to people of color.40
SSP Legal Status
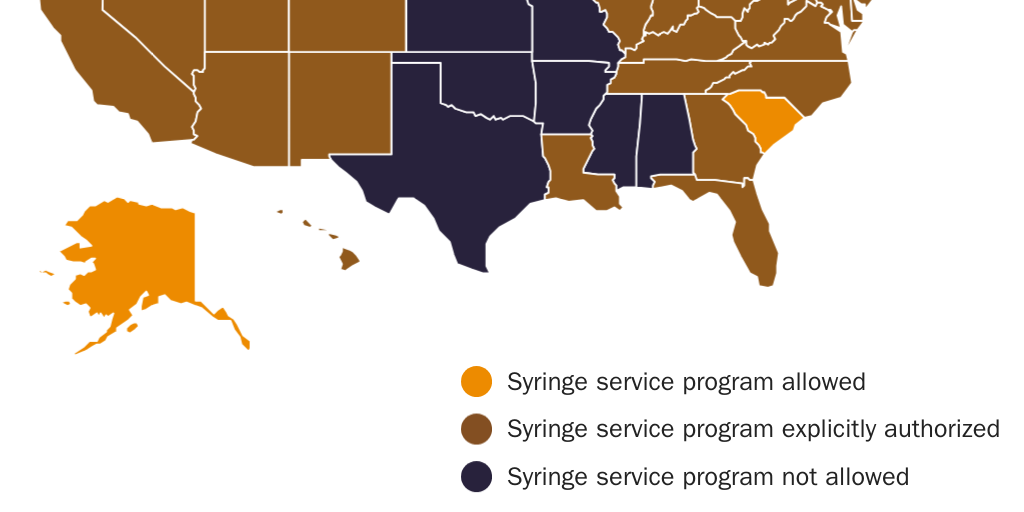
Privately funded SSPs exist in most states, including states where they are illegal. States adopt one of three approaches to SSPs: explicit authorization; tacit permission resulting from the absence of drug paraphernalia laws (as is the case in Alaska); and prohibition, often by strictly applying paraphernalia laws. Figure 3 illustrates which states prohibit SSPs, which states explicitly authorize them, and which states permit them without explicitly authorizing them. Figure 3 also shows the legal status of SSPs operating in each state and the different restrictions on how SSPs may operate. Appendix C provides more detail.
States that legally authorize SSPs impose various restrictions on their structure and operation, as well as on state-level funding opportunities. Restrictions on how SSPs operate limit their scope, hamper their success, and work against the goal of reducing the spread of disease.41 The North American Syringe Exchange Network compiles information on SSPs in most states, even states where they are illegal.42 Generally, states that authorize syringe exchanges typically exclude syringes or testing materials that SSPs distribute from any limitations on such items. Authorizing SSPs through modifications to existing paraphernalia laws tends to result in burdensome conditions. For example, some states require a one-for-one syringe exchange with individual participants, where participants must return a used syringe to receive a new syringe. Other states require the total number of syringes distributed by an SSP to equal the total number received. It also puts the legal status of possessing a syringe in question, depending on where and how a person obtained it.43 Police may assume that syringes they find on participants are illegal until the participant convinces the police the syringes were legally obtained.
States that authorize SSPs tend to place tight restrictions on how they operate or get their funding. Of the 34 states that explicitly authorize SSPs, 20 have regulations that reduce the scope, capacity, and effectiveness of SSPs. These regulations can take the form of one-for-one exchange requirements, either at the individual or program level. They can also require complicated program approval processes, have onerous data collection demands, and have narrow funding conditions.
Featured Event
Typically, a one-for-one requirement means the SSP must receive a used syringe from a client in exchange for every sterile syringe it gives out in the same transaction. Florida, Delaware, and Maine are among states that use this regulatory model. In New Mexico, a client may initially receive 30 syringes, after which all further transactions must be one-for-one exchanges. Arizona, Utah, and West Virginia all place similar restrictions on their SSPs. Distribution requirements limit the effectiveness of SSPs. Therefore, the CDC supports a need-based distribution method as opposed to strict exchanges.44
Arizona is the most recent state to authorize SSPs. The governor signed the bill into law in May 2021.45 The legislative text states, “The number of needles and hypodermic syringes disposed of through a program shall be at least equivalent to the number of needles and hypodermic syringes distributed through the program.” Commenting on the new law, Corey Davis, director of the Harm Reduction Legal Project at the Network for Public Health Law, said:
The law doesn’t require one-for-one at the level of the exchange, but it does require it at the level of the program. This would likely require SSPs to play games, like buying clean syringes and turning them in as used ones or trying to get nonclients (like diabetics) to bring their used syringes to the exchange. It [the legislation] also requires that a person [who police stop for syringe possession] claiming immunity verify that the syringe came from a program, which how the heck do you do that? But it’s a step forward.46
Onerous regulatory approval procedures for SSPs are another way to limit the functions and scope of the programs. Eighteen states require SSPs to obtain direct approval from the state government. Six states limit those who can operate an SSP to a local health department or board of health and do not allow any private entities. Many states that allow nonprofits or other independent organizations to operate an SSP require extensive consultations with other government agencies before they grant approval. In Colorado and Ohio, the boards of health will not grant approval for a new SSP without consulting with law enforcement, district attorneys, substance use disorder treatment providers, people recovering from substance use disorder, nonprofit organizations, hepatitis C and HIV advocacy organizations, and members of the community. Other states also require consultation with local health departments and law enforcement.
Various regulations and restrictions limit the effectiveness of SSPs. Some states unnecessarily require SSPs to collect personal information. California requires SSP participants to provide private information, such as “sexual behavior and history, including the participant’s self-described sexual identity, number of sexual partners in the past 30 days or six months, number of sexual partners who were also intravenous drug users, frequency of condom use, and number of times sex was used in exchange for money or drugs.” Though states promise to keep this information confidential, requiring SSPs to collect it further stigmatizes clients and may reduce participation. Some states prohibit SSPs to operate without government participation. Florida imposes a one-for-one syringe requirement that prohibits SSPs from issuing clean syringes to clients unless they surrender a used one.47 Since many users no longer possess their used syringes, that regulation prevents SSPs from distributing many potentially life-saving clean syringes. Studies show that programs with one-for-one requirements are less effective in reducing HIV and hepatitis than those without the requirement.48
Policy Recommendations
Americans have long practiced harm reduction when it comes to other drugs, including drugs that once were illegal. With the end of alcohol prohibition in 1933, makers and sellers of alcohol in the legal market became accountable for the quality of their products. Labels on alcohol products inform consumers of the alcohol content and other ingredients. Consumers of alcohol can acquire and share information about safe ways to consume alcohol. Other harm-reduction strategies include taxicabs, ridesharing services, or designated drivers to transport people who consume large amounts of alcohol.49
Because alcohol is legal and people generally view alcohol use disorder as a health issue rather than a crime, health care practitioners and the media are more comfortable informing drinkers about behaviors to avoid while consuming alcohol. Unlike policy regarding people with substance use disorders involving illicit drugs, public policy avoids stigmatizing people with alcohol use disorder. People with alcohol use disorder can anonymously seek help without fearing law enforcement and have access to myriad treatment programs. We can expect similar dynamics in a world without drug prohibition.50
As drug-related deaths and diseases continue to mount despite more than 100 years of drug prohibition, policymakers should consider proposals that shift from a zero-tolerance approach to a focus on harm reduction. Among these proposals:
- End drug prohibition. The most effective way to reduce the risks of nonmedical drug use would be for Congress and state governments to end drug prohibition. In a legal market for currently illicit drugs, drug makers and sellers would be accountable for contaminated, impure, or otherwise dangerous products. Liability laws would provide recourse to harmed consumers. Consumers would not need products to test their drugs for impurities or adulterants. Ending prohibition would reduce the risk of overdose and disease. It would allow organizations that promote harm reduction to function more effectively. With prohibition repealed, policymakers and public health officials should view substance use disorder as a health problem, not a crime problem.
- Emulate Alaska. Alaska is the only state where nonmedical drug users can gain access to the tools they need to make drug use less harmful. Alaskans can purchase syringes and obtain testing equipment without fear of prosecution. In Alaska, statewide drug paraphernalia restrictions do not impede private harm-reduction organizations. With no statewide drug paraphernalia laws on Alaska’s books, charitable and other nongovernmental organizations can implement SSPs and other harm-reduction strategies. Until federal and state drug prohibition ends, the best way to reduce the risks of harm from using drugs obtained in the illegal market is for states to repeal their drug paraphernalia laws. Eliminating state drug paraphernalia laws will let SSPs and other evidence-based harm-reduction strategies work to their full potential and, more importantly, will allow drug users to reduce harm to themselves.
- Legalize harm-reduction paraphernalia. If state legislatures lack the appetite for full repeal of drug paraphernalia laws, they should legalize drug safety testing devices such as fentanyl test strips, explicitly legalize SSPs, and make it easier for people to obtain syringes.51 The model act gives harm-reduction strategies more flexibility and freedom to innovate.
Related Video
Conclusion
It has been more than 50 years since President Richard Nixon declared a war on drugs.52 Yet, as University of Pittsburgh public health professor Hawre Jalal and coauthors reported in a 2018 Science article, “The U.S. drug overdose epidemic has been inexorably tracking along an exponential growth curve since at least 1979.”53 In November 2021, the CDC reported that annual U.S. drug overdose deaths reached a record 100,000.54 Those deaths have led federal and state lawmakers to take a fresh look at harm-reduction strategies that have been working in much of the developed world to reduce death and disease.
Unfortunately, state drug paraphernalia laws stifle harm-reduction initiatives. Only 0.22 percent of the U.S. population lives in Alaska, the only state without drug paraphernalia laws. More than 99 percent of the population lives in jurisdictions that restrict or ban various forms of harm reduction. The other 49 states and the District of Columbia must fully lift their blockades on harm-reduction efforts and allow new harm-reduction strategies to develop. They should emulate Alaska and completely repeal their drug paraphernalia laws.
Citation
Singer, Jeffrey A. and Sophia Heimowitz. “Drug Paraphernalia Laws Undermine Harm Reduction: To Reduce Overdoses and Disease, States Should Emulate Alaska,” Policy Analysis no. 929, Cato Institute, Washington, DC, June 7, 2022.

About the Authors


This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.