Scope of practice (SOP) restrictions in health care professions are often portrayed as a necessary intervention to protect consumer health and safety. Given how common this argument is, there have been surprisingly few studies trying to determine whether SOP restrictions actually have any impact on such outcomes. A new working paper seeks to fill this gap in the literature by determining whether SOP laws for certified nurse midwives (CNMs) affect health outcomes. On average, it turns out that the restrictions do not have a significant impact on maternal behaviors or infant health outcomes. Instead, they “primarily serve as barriers to practice and removing these restrictions has the potential to improve the efficiency of the health care system for delivery and infant care.”
SOP laws are determined at the state level, and regulate which activities and tasks certain professions can perform within the state. Physicians are generally unaffected, but other health practitioners are—in this case, CNMs specifically. Their level of restriction ranges from states with “no barriers,” where CNMs do not have oversight requirements, to states with “high barriers,” where they have to be under the direct supervision of a physician and may not write prescriptions. In heartening news, more states seem to be recognizing the wasteful nature of these laws. The recent trend for this specific case has been a move towards a more relaxed scope of practice environment.
Scope of Practice for Certified Nurse Midwives by State, 1994 vs. 2013
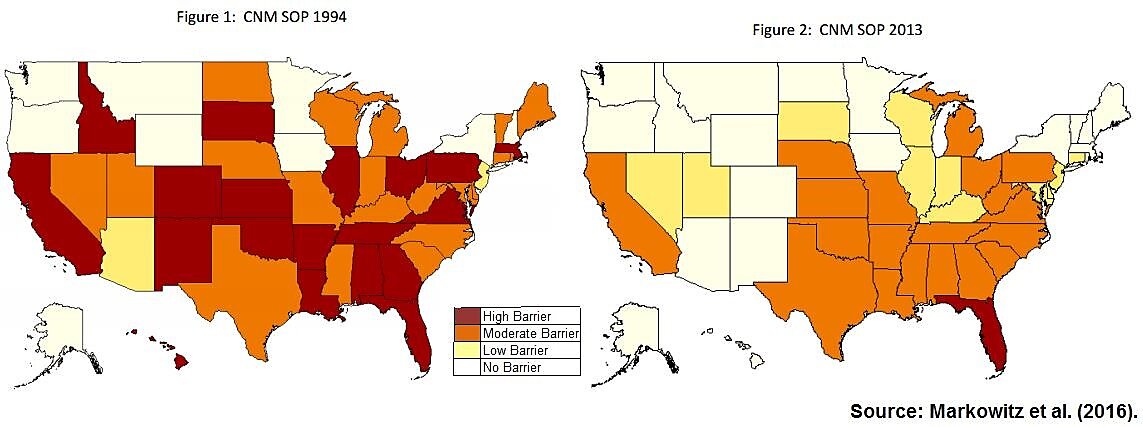
Source: Markowitz et al.
There are also differences between the states as to when such SOP laws were implemented. It is these sources of variation that allow the authors to analyze the impact of CNM SOP regulations on health outcomes. They find that states that allow for full practice by CNMs have “on average, little or no differences in maternal health behaviors or infant health outcomes as compared to states with more restrictive SOP.”
While the authors fail to find significant effects there, they do find differences when it comes to rates of labor inductions, elective labor inductions, C‑Sections, and elective C‑Sections. This has implications for overall costs in the health care system: births at delivery cost almost $40 billion in 2013, with almost half of that amount funded through the Medicaid program. As the authors note, one of the biggest drivers of the costs associated with a delivery is whether it is via C‑section. Women giving birth in “high barrier” states that are more restrictive of CNMs are 3 percentage points more likely to be induced and 1.6 percentage points more likely to have a C‑section compared to those in “no barrier” states. There are small but statistically insignificant effects when comparing states that aren’t on the two extremes of SOP restrictions. The implied savings of moving states from “high barrier” to “no barrier” exceed $85 million a year due to the resulting reduction in C‑section births.
These new findings are particularly illuminating when considered with another recent study that tried to determine whether occupational licensing in health care professions improved patient safety. Those authors looked at the licensing of midwives in the beginning of the 20th century and presented some evidence that the introduction of those laws reduced maternal mortality. It’s worth noting that the surrounding context a century ago was markedly different when it came to asymmetric information and a host of other factors. The new working paper highlighted here examines a recent situation that is more directly relevant to the discussion today, and finds that these SOP laws do not now have a significant impact on the related health or behavioral outcomes, on average.
Both studies seek to address a gap in our understanding of health care regulation, by finding out whether restrictions on practice actually improve health outcomes or consumer safety. While licensure for midwives may have had a positive effect a century ago, many things have changed in the intervening decades. Today, SOP restrictions act mostly as barriers to care. Where that’s the case, removing them could improve efficiency without harming patient safety.
