
This essay is a part of the Pandemics and Policy series.
When evaluating lessons from the COVID-19 pandemic, policymakers should recognize that
-
future novel pathogens or other crises may require very different policy responses;
-
COVID-19 inquiries would generate better “lessons for the future” if they focused more heavily on institutional flaws and pathologies that could hamper future responses to new pandemics rather than evaluating decisions over procurement or stockpiling specific to COVID-19;
-
cross‐country comparisons on pandemic preparedness, size of government, centralization of government authority, and some measures of state capacity show little correlation with excess deaths in the pandemic; and
-
since no grand theory of government appears robust in explaining pandemic performances across countries, we should be wary of those using COVID-19 to justify major increases in the size and scope of government.
The United States appears to be close to the end of the acute phase of the COVID-19 pandemic. Soon, retrospectives on this period will be written, reevaluating the country’s pre-COVID-19 pandemic readiness, the policy choices made after COVID-19 hit, and the regulatory environment around medical innovation. Already, Senators Susan Collins (R‑ME) and Robert Menendez (D‑NJ) have produced legislation calling for an independent “National Coronavirus Commission” to “investigate, identify lessons learned, and craft recommendations to improve U.S. pandemic readiness.”
In my book, Economics in One Virus, I urge that such inquiries move beyond simple delineations of “what went wrong” to instead ask “why?”: What underlying frameworks of thinking or processes drove errors that resulted in deaths or unnecessary hardship? As outlined in a previous Pandemics and Policy essay, faulty economic reasoning appears to have led in turn to avoidable policy errors that worsened the pandemic’s costs in terms of lost lives, truncated liberties, and economic destruction. These more fundamental errors of thinking risk getting lost if we focus too much on granular issues like shortages of specific medicines or vaccine inputs, which might not matter for future threats or different pathogens.

Featured Book
Economics in One Virus: An Introduction to Economic Reasoning through COVID-19
Economics in One Virus draws on the dramatic events of 2020 to bring to life some of the most important principles of economic thought. Packed with supporting data and the best new academic evidence, those uninitiated in economics will be given a crash course in the subject through the applied case study of the COVID-19 pandemic to help explain everything from why the United States was underprepared for the pandemic to how economists go about valuing the lives saved from lockdowns.
But we also should not presume that COVID-19 outcomes are simply a function of the specific public health policies implemented in response to the virus. As economist Wendy Carlin and others have noted, a pandemic’s impact is determined not only by the pathogen’s features and government-led public health efforts but also by the social networks, civil society institutions, and the social norms of the population it penetrates.
Even for countries that adopted substantially similar COVID-19 policies, we have learned that process sometimes matters as much as substance. The speed of policy implementation or the degree of precaution embedded in government agencies has led to big differences in timing on everything from testing availability to the rollout of vaccines.
Identifying more general weaknesses in decisionmaking, sources of bureaucratic dysfunction, and reasons for a lack of overall societal resilience to this shock are therefore much more fruitful endeavors for informing future choices than re-running COVID-19-specific mistakes.
This type of analysis presents a new danger, however. Intellectuals, politicians, and commentators have already been using this experience to push for broader policy overhauls that they have long desired. My former colleague Kristian Niemietz, writing in a UK context, has described this as “coronfirmation bias”—a type of confirmation bias that says the experience of the pandemic justifies the urgent need for reforms that the advocate has always sought.
In the United States, this bias has mainly materialized in claims that the pandemic justifies new government programs or ‘investments.’ The argument is invariably that previous government inaction or failures to spend more left the country structurally more vulnerable to COVID-19 than it should have been.
Prominent commentators have told us that the high death toll from COVID-19 highlights inadequate U.S. preparation for pandemics, as well as the lack of a bigger social safety net, the limits of federalism, and an overall weakness in U.S. “state capacity.” Yet looking at data across Organisation for Economic Co-operation and Development (OECD) countries, none of these supposed prerequisites appear to be necessary conditions to achieving much better public health performances than the United States experienced. In fact, almost all the major “grand narratives” about how the size and scope of the U.S. government hindered the pandemic response fall apart in cross-country comparisons.
For sure, one must be careful not to derive overly strong conclusions from cross-country comparisons. Examining public health outcomes across nations against individual variables risks hiding how some specific additional spending—on, say, hospital capacity or personal protective equipment—may have helped insure against the worst outcomes in particular places, such as when hospitals risked being overrun. This would not show up in broad-brush correlations. At the very least, however, the absence of any meaningful correlations provides ground to stop and think before reaching for grand narratives on how this crisis proves the need for bigger, more centralized government.
The rest of this essay analyzes such claims by looking at cross-country COVID-19 mortality and excess death outcomes alongside various measures of the size and scope of government. The key takeaway is that much of the conventional wisdom on what would have helped the United States in the pandemic is not borne out by the examples of countries that, thus far, have handled this crisis better in public health terms than we have.
Pandemic Preparedness
“We just weren’t well prepared for the pandemic.” How often have we heard a variation of that said over the past year? The problem is that before COVID-19, international assessments of “pandemic preparedness”—most notably the 2019 Global Health Security Index (GHSI)—suggested that the United States was the best prepared country in the world to face a novel pathogen.
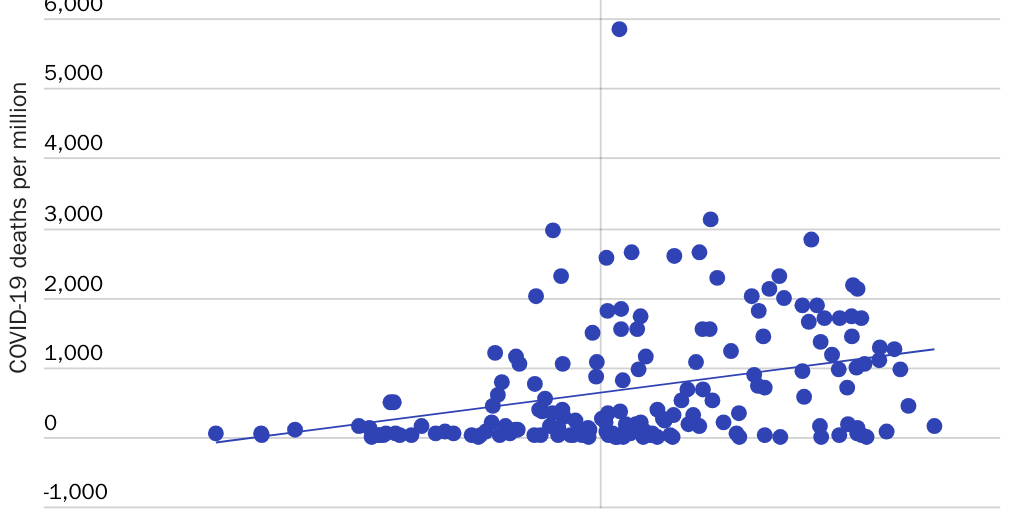
That index has proven a terrible predictive guide to how well countries have dealt with COVID-19 so far. As Figure 1 shows, there is no meaningful correlation between OECD countries’ pandemic preparedness scores and COVID-19 deaths per million—with a very mildly negative correlation overall now that was mildly positive for most of 2020.
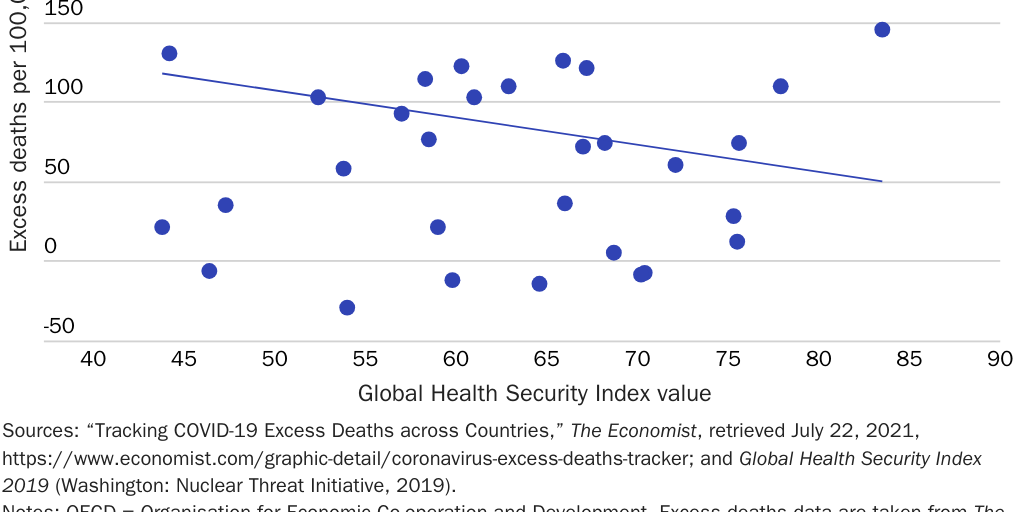
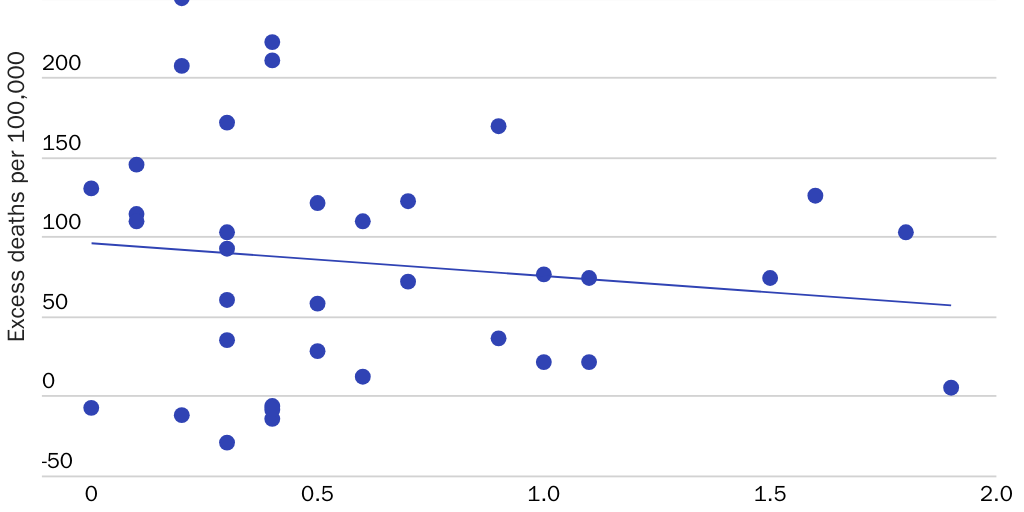
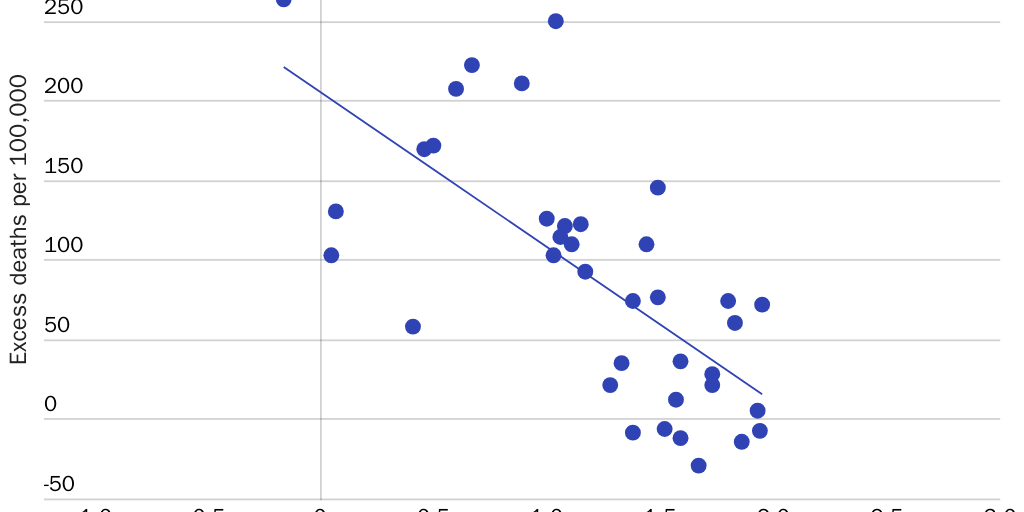
Since official COVID-19 deaths have been tallied according to different criteria across countries, “excess deaths” in the pandemic may be regarded as a more reliable guide to a country’s overall handling of this public health crisis. Figure 2
similarly shows only a modest negative correlation between the GHSI preparedness value for a country and excess deaths per 100,000 people per year for OECD countries (see note under Figure 2).
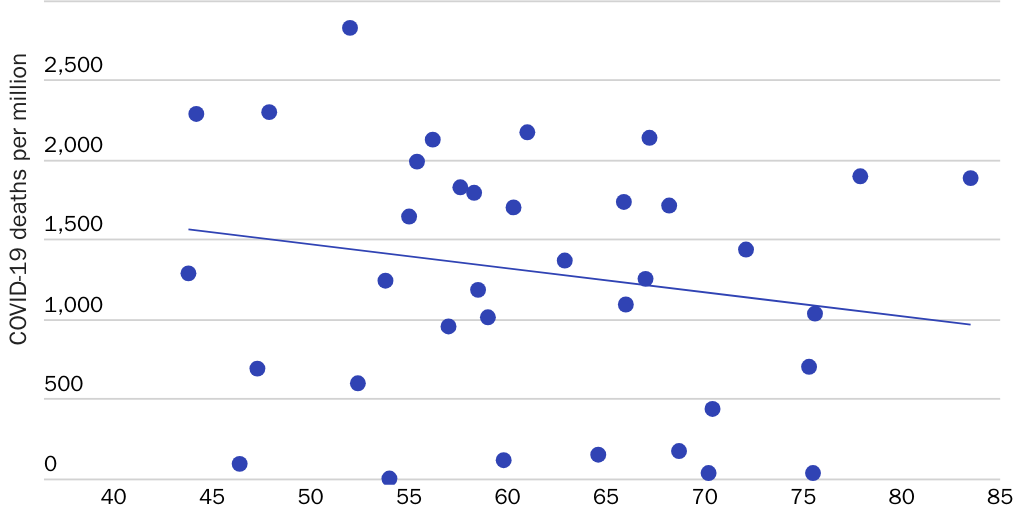
The index ranked the United States the best prepared country in the world overall, followed by the United Kingdom and the Netherlands. The United States, it said, led the world in “early detection and reporting,” was second only to the UK for “rapid response and mitigation,” and number one for the sufficiency and robustness of the health care system in treating the sick and protecting health care workers.
And yet, as of July 22, 2021, the United States had seen 1,879 COVID-19 deaths per million and the UK 1,888 deaths per million, compared to 6 deaths per million in Singapore (24th on the preparedness index), 5 per million in New Zealand (35th on the index), and 87 per million in Iceland (58th on the index).
One reasonable conclusion that might be drawn from the GHSI’s lack of predictive power is that it was poorly designed. For example, the index marked down countries that had restricted travel in the past year because of an infectious disease threat. Perhaps a better methodology that was not predicated on “box checking” for grading “preparedness” would have better predicted disease outcomes.
To be fair, the GHSI couched its relatively glowing assessment of U.S. readiness with the caveat that “no country” was “fully prepared for epidemics or pandemics” and explicitly said that “international preparedness” overall was poor. Before the pandemic, a host of experts on infectious diseases echoed this point, emphasizing that relatively little was spent on this aspect of public health compared with national defense and the financial system, despite the potential for huge loss of life and economic disruption from a novel pathogen.
But electoral incentives tend to push against investing in preparation for low-probability, high-risk events like pandemics, because politicians get rewarded for day-to-day spending and relief, not investments in public goods that the public does not see.
It’s only when the political salience of pandemics is high that political leaders have adequate incentive to prepare for the future. Thus, it shouldn’t be surprising that South Korea and other countries that experienced SARS and MERS outbreaks reacted more quickly to the initial COVID-19 outbreak than other countries. Perhaps true preparedness comes from learning by experience and cannot be assessed easily beforehand.
Certainly, President Biden seems to think that we have suffered the cruel consequences of past deficiencies in preparation. His administration’s budgeting priorities originally proposed an extra $30 billion in spending on pandemic preparation over the next four years, including more funds for the Strategic National Stockpile, tests and treatments, prototype vaccines, and first-responder training. The implicit message was that there wasn’t enough preparation or investment in pandemic readiness “public goods” before COVID-19 hit.
But an alternative assessment of the index’s predictive failure is less comforting. Perhaps measurable “preparedness” is just not as important as we might think in determining outcomes once a pandemic begins. Instead, public health outcomes may turn on highly specific, consequential decisions on things like testing or vaccines rather than measurable disease-fighting “capacity” or the protocols in place beforehand.
Former Food and Drug Administration (FDA) commissioner Scott Gottlieb, for example, has acknowledged that the U.S. COVID-19 response was hampered by public health authorities’ focus on preparing for an outbreak of influenza rather than a coronavirus. It’s possible that South Korea and others just got “lucky” that their past MERS or SARS experiences and specific early decisions stood them in good stead for this virus despite objectively worse preparedness for pathogens overall.
Over some dimensions, at least, it’s obvious that bad decisions, rather than a lack of preparedness, was the problem. The United States scored 100/100 in the GHSI sub-index for “capacity to test and approve new counter measures.” It has plenty of labs that could theoretically undertake diagnostics tests, and the FDA has emergency authority to skirt the usual rules and quickly approve them. Yet it’s widely acknowledged that the FDA delayed diagnostic tests through its Emergency Use Authorization procedure, worsening outcomes early on by reducing the possibility of identifying infectious individuals. Here, bad decisions, rather than a lack of pandemic readiness, were key.
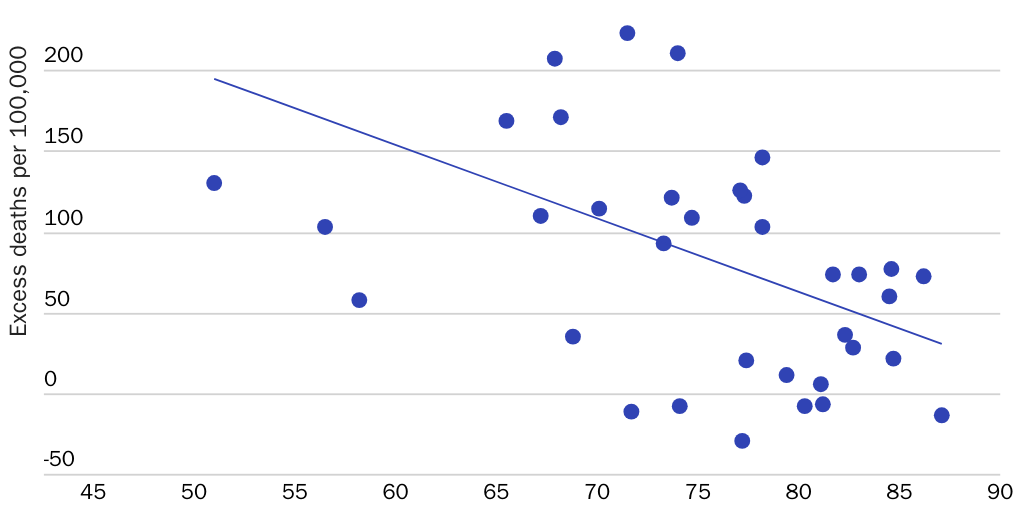
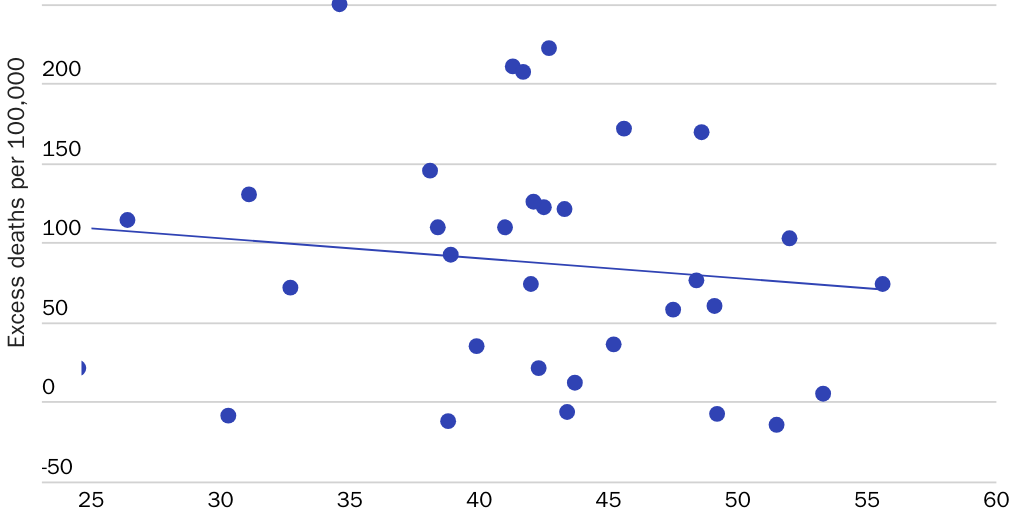
Another indicator suggesting that “pandemic preparedness” is overrated is the fact that scoring well on the index sub-component “overall risk environment and country vulnerability to biological threats” seems to be correlated more strongly with fewer deaths than the overall preparedness index (see Figure 3).
This sub-index includes variables not really linked to pandemic-specific preparation, including broad poverty levels, physical infrastructure quality, risks of social unrest, and even trust in government. Unlike, say, merely having a “national public health emergency response plan in place which addresses planning for multiple communicable diseases” and making it publicly available, these risk environment variables defy quick policy “fixes”: there’s no simple policy “lever” to pull that addresses these thornier, structural challenges.
For all these reasons, we should be wary of confident assertions that the crisis proves the need for massive new investments in pandemic preparedness. If we were able to judge what future capacities would help ameliorate pandemics’ effects, then given the staggering costs of a global pandemic, investing modest amounts could pay handsome long-term dividends. But the failure of the GHSI suggests that even experts find it hard to assess what types of preparedness are necessary before we know the contours of a crisis and the features of a pathogen, while much preparation and capacity building can prove useless in the face of bad decisions.
The Safety Net
Another claim made early in the pandemic was that the United States would suffer poor COVID-19 outcomes because of its “inadequate” social safety net. Without generous support to insulate households from the disruption, it was said, people would lack the financial incentive to self-isolate: they’d have to keep working, which would worsen community spread.
In reality, of course, after states implemented lockdowns, the federal government quickly passed a massive stimulus package in the form of the Coronavirus Aid, Relief, and Economic Security Act, which included huge expansions of unemployment insurance benefits, direct-to-household checks, expanded child tax credits, and payroll support via the Paycheck Protection Program. European countries differed in their approach, but many passed novel furlough schemes to keep laid-off workers attached to firms while shuttering large parts of their economies.
Given the observed flexibility exhibited in shoveling trillions of dollars out the door quickly, why would we think that there were any lessons from this crisis about how permanent government welfare policies would affect public health outcomes? In fact, across OECD countries there is virtually no correlation whatsoever between excess deaths and pre-pandemic spending on cash benefits as a percentage of gross domestic product (GDP), nor between excess deaths and pre-pandemic unemployment benefit spending (see Figures 4 and 5).
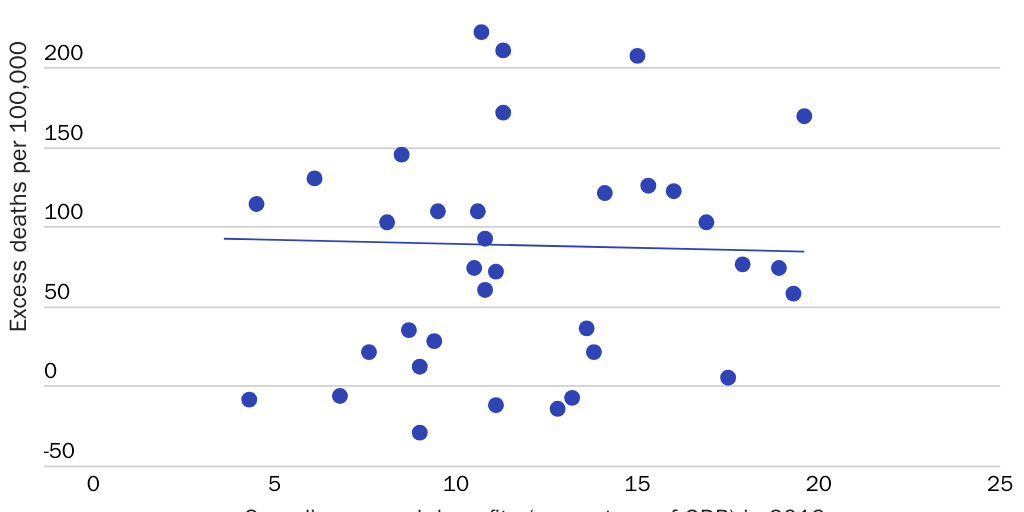
You don’t need a scatterplot to inform you that a redistributive welfare state was no guarantee of good public health outcomes during this pandemic. Countries such as Italy and Poland spend much more on cash benefits than the United States but have seen worse outcomes on excess deaths. Other countries that spend far less than the United States, such as South Korea and Taiwan, performed much better. None of this experience indicates any useful lessons about what the level of various U.S. social welfare benefits should be.
That hasn’t stopped politicians and public intellectuals from insisting that the pandemic proves the need for a more permanent lavish social welfare state.
Apparently, the $600 weekly supplemental unemployment insurance benefits, the stimulus checks, and more “only highlight the inadequacies of the regular unemployment insurance system” and other problems with the “moth-eaten,” “ill-funded labyrinthine system rife with arcane eligibility criteria.” Economist Daron Acemoglu has said that a key lesson of this crisis is that we need a “much better social safety net.” Advocates, commentators, and former politicians have suggested that the crisis highlights the virtues of a universal basic income.
To be sure, the U.S. federal welfare state has huge, well-documented problems, which create all sorts of perverse incentives. We’ve seen significant indications of waste and fraud as the federal government threw money around, and some have argued convincingly that unemployment insurance benefits only had to be made extremely generous precisely because states did not have the institutional capacity to deliver something more economically sensible (say, with benefits provided as a proportion of previous income).
But when thinking about welfare, we must distinguish program administration from benefit levels. The idea that the size of the benefits considered appropriate in crisis conditions holds lessons for “normal” welfare provision is misguided. A time when you are knowingly shuttering much of the economy, and seeking to prevent resulting hardship, is one in which you might care less about work disincentives or other perverse tradeoffs. All those problems come flooding back in “normal” times.
Size of Government
Others have argued that the pandemic proves the need for a more supportive government in general, in areas ranging from universal health care to aggressive industrial policy.
A Time magazine article in April 2020 summed up a vocal minority opinion when it said that the “Covid-19 crisis makes utterly clear why some problems demand big government solutions, and why they can’t just be temporary.” In the London Review of Books, Pankaj Mishra contrasted the Anglo-American “ideologies of unfettered markets and minimal government” with the state-building instincts of South Korea and Germany.
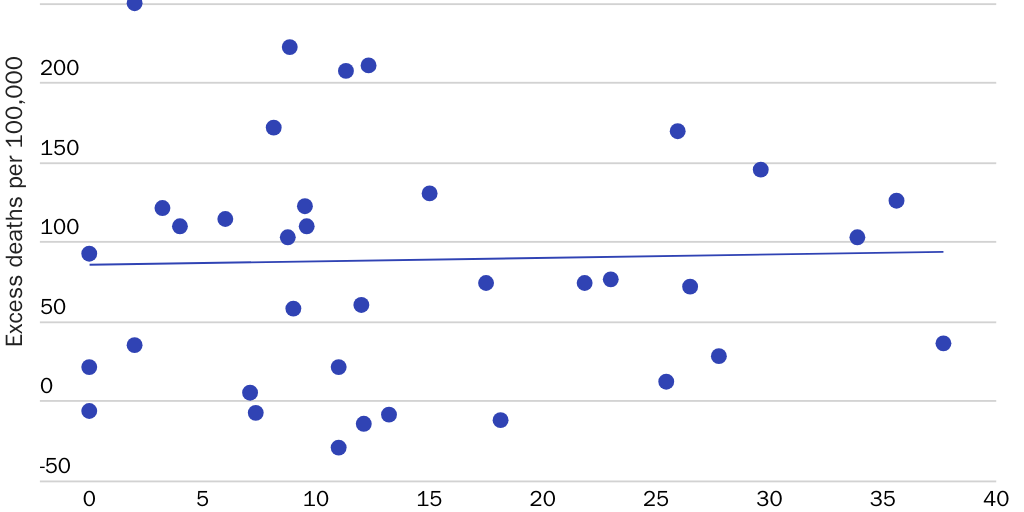
So how does the overall size of government—proxied for by government spending as a percentage of GDP—line up with COVID-19 outcomes? As you can see in Figure 6, once again, there is barely any correlation.
That’s not surprising. As Kristian Niemietz has argued, to the extent the government can affect health outcomes, a pandemic is mainly a test of specific capabilities: public health decisions, health care capacity, pandemic-associated welfare supports, and a state’s ability to enforce its laws. There’s little reason to think those capabilities track very well with the overall size of government in nonemergency conditions.
That countries with significantly lower government spending as a share of economic output than the United States (38.1 percent of GDP in 2019), such as South Korea (30.3 percent), Switzerland (32.7 percent), and Ireland (24.5 percent), have seen much better outcomes in this crisis suggests that having a bigger government beforehand is not a necessary condition for better public health outcomes in a pandemic. To the extent particular additional spending might have mattered, this suggests focus should center on the priorities of government, not its overall claims on the private sector.
Nor can differential cross-country performances be explained by recent deficit reduction, dubbed ‘austerity’ by its opponents. Some countries that saw high levels of excess deaths, such as Lithuania, Portugal, and Slovenia, had indeed seen big increases in their real primary surplus between 2011 and 2019, according to the International Monetary Fund—so, significant deficit reduction. But Japan and Greece had slashed their deficits over the past decade, yet saw a much better public health performance in the pandemic. The United States and the UK have suffered similar excess death levels, despite the latter fiscally tightening since 2011 and America not.
Even looking at the change in government spending as a proportion of GDP between 2011 and 2019 holds no clear lessons for the pandemic. Six European countries that saw government spending fall by more than 7 percentage points of GDP were Lithuania, Slovenia, Portugal, Greece, Iceland, and Denmark. The first three have so far seen extraordinarily high excess deaths in the pandemic; but Greece, to date, has seen low levels of excess deaths, while Icelandic and Danish death levels, surprisingly enough, have been below levels seen in previous years.
Whatever else explains the high numbers of excess deaths in some countries, small or shrinking government is not the cause.
Federalism: Feature or Bug?
Perhaps a more intuitive claim is that in emergencies such as pandemics, the decentralized power inherent within a federal system of government can hinder a coordinated public health response. That’s certainly been the conventional wisdom in much U.S. debate. A Time magazine article in 2020 argued, for example:
Countries that have mounted a strong, centralized response—South Korea, Germany, China—are doing a better job containing the virus, and therefore saving li[v]es, than those that have not. This comes as no surprise to most epidemiologists. Few local/state governments have the capacity to mobilize the necessary resources, and—since viruses don’t respect political boundaries—the broader the response, the more likely it is to work.
That seems reasonable. But does this intuition scale? It’s trivially true that “good” policies, centrally administered, might have improved outcomes. And clearly, coordination to break circuits of transmission of a novel pathogen, if executed at the right time, could have averted many deaths.
This argument relies on the assumption, however, that the centralized authority of the federal government would have made the right calls at the right time. The flipside of centralizing power is that you risk entrenching systemic mistakes. How do we know, for example, that the federal government would not have made the mistake of seeding nursing homes with COVID-19 patients, as happened in New York, across the whole country? What if the sorts of inadequacies seen at the FDA were replicated across other agencies that had states’ current powers? That some U.S. states have performed much better than others suggests that there’s nothing inherent in a more localized approach that necessitates bad outcomes.
Indeed, it’s difficult to square any theory that celebrates the efficacy of centralized power with claims (often from the same people) that former president Donald Trump was responsible for hundreds of thousands of U.S. deaths in 2020. Just who do they think would have been in charge in a unitary, centralized United States for the pandemic?
True, some countries with extensive regional autonomy have had dreadful COVID-19 public health outcomes—notably Italy, Spain, and Belgium. Then again, Germany, Switzerland, Canada, and at least early on, Australia, all with high degrees of decentralized regional authority, have seemingly coped much better.
At the other end of the spectrum, political centralization has certainly provided no guarantee of good outcomes either. The UK is incredibly centralized, especially when it comes to public health powers, but so far it has had a higher COVID-19 death toll than the United States.
Ideally, there would be some sort of index of public health–related centralization to begin assessing whether regional autonomy helped or hindered public health efforts during the COVID-19 pandemic. As far as I am aware, no such measure is yet available. However, as Figure 7 shows, more conventional measures of regional authority for OECD countries do not correlate with COVID-19 excess death rates.
Conceptually, there are no doubt instances where better replications of policies across states could have improved public health policy in this pandemic, especially early on. We saw a bottom-up process, for example, of northeastern states, as well as Virginia, Maryland, and Washington, DC, coordinating to neuter the risk of the disease spreading across their porous borders.
But too much centralization risks losing the advantages of local experimentation and setting policy closer to within-state needs. Moreover, evidence shows that local COVID-19 restrictions have substantial spillover effects anyway, eliciting behavioral responses in nearby areas. This further diminishes the potential benefits of greater centralization at a national level.
Overall, there is little cross-country evidence to suggest that greater centralized authority was crucial to improving public health outcomes for the United States, let alone broader economic and social outcomes.
State Capacity
Luminaries including economist Tyler Cowen and Francis Fukuyama have claimed that U.S. failures in the pandemic can, at least in part, be explained by weak or insufficient “state capacity.” As Massachusetts Institute of Technology’s Daron Acemoglu put it recently:
Even more ominous, in my opinion, is that the pandemic hit the fault line created by the erosion of state capacity. The most jarring aspect of this is the Centers for Disease Control and Prevention, which is the first, second, and third line of defence in the US against pandemics and infectious diseases. This is an institution with an illustrious past, which regularly got full marks for how quickly it dealt with problems.… This comes from the incompetence of the Trump administration combined with the erosion of state capacity and the demoralisation and disempowerment of institutions.
State capacity is a rather ill-defined term, but measures of it aim to quantify the ability (or capacity) of governments to deliver public goods or achieve their other policy goals.
This is usually proxied for by various structural measures being combined into an index, such as the soundness of a country’s institutions, the state’s extractive power (usually its tax-raising capacity), and measures of government effectiveness or bureaucratic quality.
U.S. state and federal governments have clearly failed in many regards in this pandemic. But is that due to deficient “state capacity” or the result of bad decisions and misguided priorities? To paraphrase economist Bryan Caplan: Can a federal government that has approved $6 trillion in new pandemic-related “stimulus” in just over a year, and state governments that shuttered much commercial activity, really be considered lacking in “capacity”?
Economist Ryan Murphy and coauthors produced a comprehensive country-by-country state capacity index measure prior to the pandemic. The index combines measures of “the rule of law, the authority of the state over its territory, the rigorousness and impartiality of public administration, whether public expenditures are on particularistic or public goods, the modernity of the state’s source of its revenue, and the universality of the provision of education.”
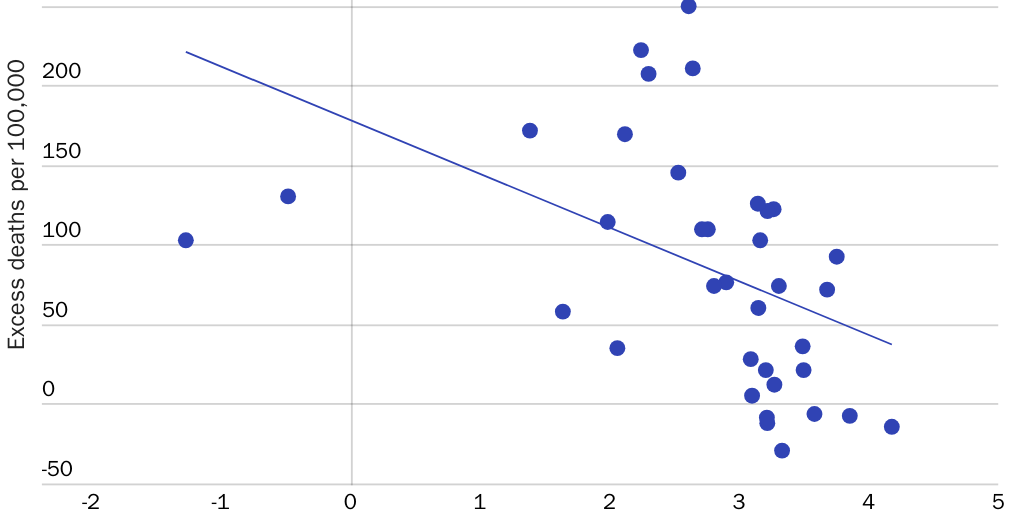
On the face of it, their results show that higher state capacity does not guarantee relative success with COVID-19. Some high-scoring countries such as South Korea (3.2 score for its comprehensive state capacity measure), New Zealand (3.5), and Switzerland (3.7) have indeed fared better on excess deaths than the United States (2.5). But countries such as Greece (1.6), Israel (2.1), and Chile (2.0) have performed better than the United States so far despite weaker state capacity on this measure.
However, as Figure 8 shows, for OECD countries overall, there does appear to be a relatively strong negative correlation between the index and excess deaths (i.e., countries with higher state capacity do tend to have seen fewer excess deaths). This relationship doesn’t hold across all countries (see Figure 9), but perhaps that’s to be expected: the huge demographic differences across developed and developing countries, and perhaps the lack of accurate death counts in many of the latter, are likely to muddy any correlation.
A different measure used sometimes as a proxy for state capacity is the World Bank’s “government effectiveness” index, which incorporates variables capturing “the perception of the quality of public services, the quality of the civil service and the degree of its independence from political pressures, the quality of policy formulation and implementation, and the credibility of the government’s commitment to such policies.” As Figure 10 shows, there is again a strong negative correlation between this index and excess deaths at this stage of the pandemic.
Intriguingly, this relationship is driven by relatively recent events: a similar analysis from economists at the Federal Reserve Bank of St. Louis in November 2020 found no apparent relationship between these variables. Such a sharp adjustment is consistent with the view that a lot of developed countries that thought they had “effective” governments failed to take rapid preventive actions in the early stages of the pandemic. Over time, however, countries with less-effective governments suffered later outbreaks or saw worse outcomes as those with more-effective governments got their acts together.

Featured Event
The Economics of Lockdowns
The COVID-19 pandemic has had dire effects on both public health and the economy. In reaction to the virus’s spread, many states have implemented stay‐at‐home orders and closures of all “nonessential businesses.”
Even so, there’s reason to wonder whether measures of state capacity or government effectiveness tell us anything particularly meaningful about a country’s likely outcomes in a pandemic. It’s worth noting that of several hundred factors that influence a country’s score on the Government Effectiveness Index, only around 20 could be said to be directly related to pandemic preparedness and public health, while 60 more have indirect impacts, if any. The possibility of spurious correlations is therefore high.
In addition, as with the Global Health Security Index, performing “better” on dozens of the World Bank’s variables could conceivably raise a country’s government effectiveness rating while harming its ability to counter a pathogen. For example, countries with highly regulated labor markets and restrictive border policies were ranked down in the index. Yet, timely border closures before the pathogen had arrived, as well as an ability to enforce workplace safety protocols, are now widely seen to have been necessary to mitigate COVID-19 transmission, however much they might be undesirable ordinarily.
Even if there currently appears a robust relationship between state capacity or government effectiveness and public health performance, it’s not clear that relationship will persist. Three countries not near the top for state capacity or government effectiveness among OECD countries—Israel, the United States, and the UK—led the way on early vaccinations, meaning 61 percent, 48.5 percent, and 54.2 percent of their overall populations were fully vaccinated by July 22. Though these countries are now struggling with the Delta variant, it seems likely that all will see improved excess death performances for the coming months relative to countries with much weaker vaccination coverage and Delta outbreaks.
Consider several OECD countries in the top half of the state capacity index that also have low excess deaths to date: New Zealand has fully vaccinated just 13.6 percent of its population, Australia 12.1 percent, Japan 24.9 percent, and South Korea 13.3 percent. It’s conceivable that these countries will face more challenging public health environments in the coming months, particularly with the Delta variant. This could worsen their excess death figures. Even if they do ward off deaths through other mitigation or suppression measures, these might come at a much higher economic cost than in the highly vaccinated countries.
Perhaps the best we can say is that, on average, in a protracted pandemic, developed countries with good institutions tend to see better public health outcomes in the medium term, although this could look quite different over time, dependent on decisions and logistical challenges, such as vaccine rollouts.
Given that countries such as Israel have done so well on rolling out vaccines, in fact, it does raise the question of how accurate these state capacity or government effectiveness indices are as true indicators of states’ abilities to get things done or harness resources effectively. We are back to the same issue we saw with the pandemic preparedness index: Does not the pandemic show the limitations of these box-checking assessments of capacity?
Certain commentators, such as British policy journalist Jon Stone, have even suggested that the country’s overall performance with COVID-19 is itself a good indicator of state capacity—given that the pandemic was a test of different states’ ability to both harness resources and provide public goods under pressure. But as a guide to thinking through policy implications, this borders on circularity:
“What caused our poor COVID-19 performance?”
“Lack of state capacity!”
“How do we know we have a lack of state capacity?
“Our COVID-19 performance.”
State capacity surely only has use as a meaningful concept if it can measure a state’s capacity to do things ex ante. And, clearly, outcomes in this pandemic have been affected by past experiences, decisions by leaders and public health experts, and other societal phenomena that are also unrelated to the capacities of the state.
While there is some evidence suggesting that objectively assessed state capacity might be related to public health performance in this pandemic, then, anyone using a lack of it to explain the United States’ poor outcomes should be asked to provide more detail on what specific capacity U.S. governments lacked and the mechanism through which this “capacity” could be realistically improved. As we’ve seen, a bigger government overall doesn’t translate into a better pandemic response.
Conclusion
At various stages of this pandemic, commentators have advanced grand narratives about the causes of the high excess death toll in the United States, linking bad outcomes to a lack of government activity or an insufficient centralization of government power.
Few in politics are free from the temptation to “never let a crisis go to waste” by invoking the pandemic to justify policies they’ve always favored: a bigger military, the Green New Deal, or more protectionist trade policy.
But some of the state-centric narratives are more beguiling. If only we’d prepared better, or had higher social welfare spending so people would isolate without financial fear, or spent more on helpful government programs, or had a stronger federal government coordinating policy nationwide, or took “state capacity” more seriously, surely we’d have seen fewer deaths and less damage to our economy in this pandemic?
The evidence presented here suggests that we should be skeptical of these assertions. While careful retrospectives may indeed find useful, generalizable policy lessons from all this, the cross-country experience with COVID-19 offers little support for the notion that a more expansive, powerful, or centralized U.S. federal government would have handled this pandemic better.
About the Author


This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.